
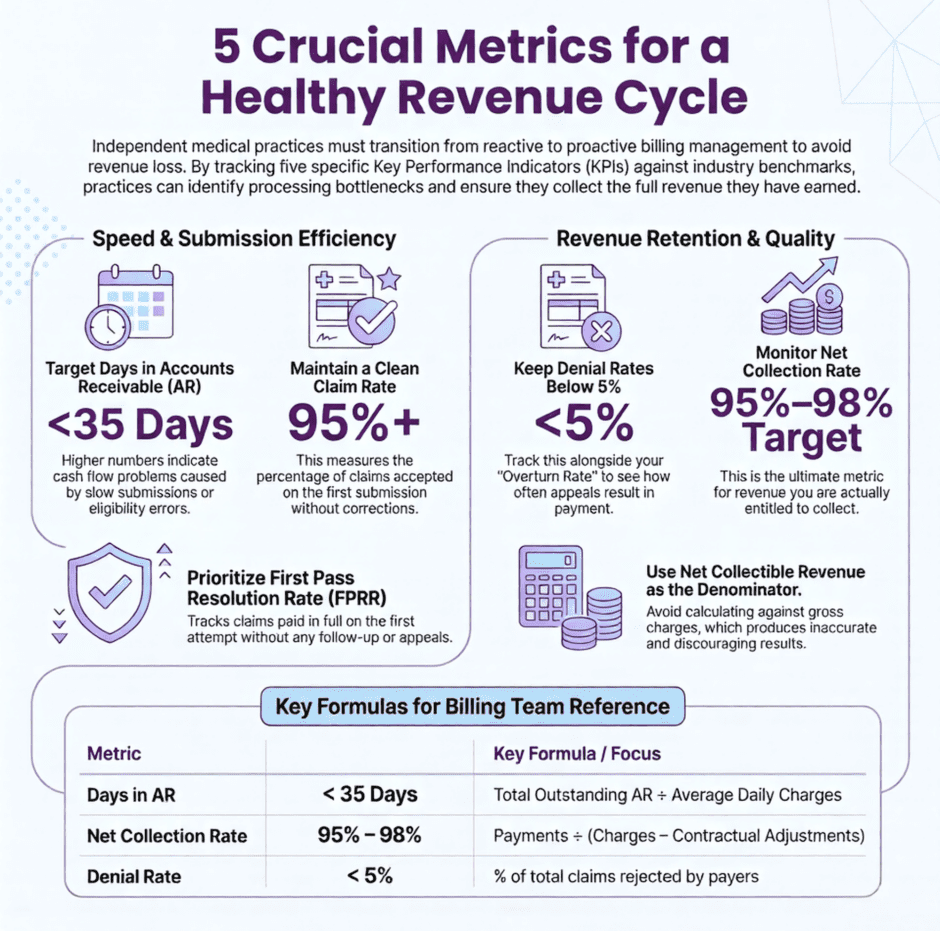
The revenue cycle metrics that matter most for independent practices are clean claim rate, first-pass resolution rate, days in accounts receivable, denial rate, and net collection rate. Each one measures a different point of failure in the billing process, and together they give a practice an accurate picture of where money is being lost and why.

Independent providers operate with tighter margins than health systems and have far less capacity to absorb revenue loss from inefficiency. A denial rate above 5%, days in AR consistently above 40, or a net collection rate below 95% are all signals that something in the billing workflow needs attention. In a solo or small group practice, those gaps compound quickly because there is no volume to offset them.
This article defines each of the essential RCM metrics, explains what the benchmarks look like for independent practices specifically, and describes what tends to drive performance in the wrong direction when these numbers start to drift.
The Five Metrics That Show Performance Problems First
1. Days in Accounts Receivable
Days in AR is one of the most widely used revenue cycle metrics, and for good reason. It tells you, on average, how many days it takes to collect payment after a claim is submitted. The calculation is straightforward. Divide your total outstanding AR by your average daily charges.
The industry benchmark for most specialties is under 35 days. If your number is sitting at 50 or 60 days, that’s not just a billing inconvenience. It’s a cash flow problem. Money you’ve already earned is sitting uncollected, and the longer it sits, the harder it becomes to collect.
High days in AR usually point to one of a few root causes: slow claim submission after the date of service, eligibility errors that cause initial rejections, or inadequate follow-up on unpaid claims. Each of these has a different fix, which is why knowing your days in AR is just the starting point. You have to dig into why it’s high before you can bring it down.
2. Clean Claim Rate
Your clean claim rate is the percentage of claims that get accepted and processed by the payer on the very first submission, without any corrections or resubmissions needed. It’s one of the clearest indicators of how well your front-end billing processes are working.
The target is 95% or higher. If you’re below that, you’re generating unnecessary administrative work every time a claim bounces back, and you’re delaying payment by days or weeks on a significant portion of your volume. Common culprits include patient eligibility not being verified before the visit, incorrect provider information on the claim, missing or mismatched diagnosis codes, and authorization numbers that weren’t captured at the front desk.
A low clean claim rate is fixable, but it usually requires looking at processes that happen before the claim is ever submitted, not just in the billing department.
3. Denial Rate
Your denial rate is the percentage of claims that payers reject after submission. The industry benchmark is under 5%. If you’re above that, you’re losing revenue on claims that you should have been paid for, and you’re spending staff time on appeals that could have been avoided.
Denial rate alone does not tell the complete story. The denial rate alone doesn’t tell you enough. You also need to know your denial overturn rate, which is how often your appeals actually result in payment. A practice with a 10% denial rate but a 90% overturn rate is in a very different position than one with a 10% denial rate and a 40% overturn rate. Track both numbers together for a complete picture.
4. Net Collection Rate
Net collection rate is the single most accurate measure of whether a practice is capturing the revenue it is entitled to collect. Your net collection rate tells you what percentage of the money you were actually entitled to collect, after contractual adjustments, you actually collected. The formula is, payments divided by charges minus contractual adjustments, expressed as a percentage.
The benchmark is 95 to 98%. Anything below 95% means money is leaving your practice through write-offs, untimely claim submissions, or patient balances that never got collected. The gap between what you should have collected and what you actually collected is real revenue that’s gone for good.
Practices that calculate this metric against gross charges rather than adjusted charges produce a figure that understates actual performance significantly.
5. First Pass Resolution Rate
First pass resolution rate, sometimes called FPRR, is closely related to clean claim rate but measures a slightly different thing. It tracks the percentage of claims that are paid in full on the first attempt, without any follow-up, resubmission, or appeals process needed.
This metric is a direct measure of billing efficiency. A high FPRR means your billing team is spending time on new claims, not constantly chasing old ones. A low FPRR is a warning sign that your team is spending the majority of their time in reactive mode, which is exhausting and expensive.
Reading Your AR Aging Report
The AR aging report breaks your outstanding claims into time buckets based on how long they’ve been unpaid. Most practice management systems generate this report automatically, but a surprising number of independent practices don’t review it regularly.
Here’s what each bucket is telling you:
- Zero to 30 days is normal. Claims in this range are still within the standard processing window for most payers. No action needed beyond routine monitoring.
- 31 to 60 days needs attention. These claims are taking longer than expected and should be actively followed up with payers to confirm receipt and status.
- 61 to 90 days requires escalation. Something has gone wrong with these claims, whether it’s a denial that wasn’t caught, a payer processing delay, or a missing piece of information. Each one should be individually reviewed.
- 90-plus days is where revenue is genuinely at risk. Most payers have timely filing limits, and claims approaching those limits need to be prioritized immediately. Claims that have already passed timely filing are generally uncollectible and need to be written off.
The 90-plus day bucket is often where independent practices are quietly losing the most money. Reviewing it monthly and setting a clear policy for how to handle aging claims is one of the highest-return activities an independent practice billing team can do.
Denial Management: Fixing the Leak, Not Just Mopping the Floor
 Denials are frustrating, but they’re also informative. Every denial reason code is a data point that tells you something about where your process is breaking down. The problem is that most independent practices treat denials as individual events to be resolved rather than patterns to be analyzed and eliminated.
Denials are frustrating, but they’re also informative. Every denial reason code is a data point that tells you something about where your process is breaking down. The problem is that most independent practices treat denials as individual events to be resolved rather than patterns to be analyzed and eliminated.
The most common denial reasons in independent practices tend to cluster around a short list of issues. These include eligibility not being verified before the visit, prior authorizations that weren’t obtained or weren’t documented correctly, diagnosis codes that don’t support the service billed, and claims submitted after the payer’s timely filing window closed.
None of these are random. They’re all process failures that happen at specific, identifiable points in the patient encounter workflow. Fixing a denial root cause doesn’t just recover one payment. It prevents the same denial from happening on every future claim with that same issue.
Building a simple denial log, even a basic spreadsheet that tracks denial date, payer, reason code, and resolution, gives you the data you need to see patterns. Once you can see that 40% of your denials are coming from one payer for one specific reason, you have a target. Without that data, you’re just working through a pile of problems with no way to tell which ones matter most.
Coding Accuracy: The Metric That Lives Upstream
Every other revenue cycle metric is downstream of coding. If your codes aren’t accurate, your claims won’t be clean, your denial rate will be high, and your net collection rate will suffer. Coding accuracy is the foundation that everything else rests on.
For independent practices, the most expensive coding errors tend to happen with E/M codes. Undercoding is more common than most providers realize because physicians often default to a lower code level to avoid the appearance of upcoding. But routinely billing a 99213 for a visit that genuinely supports a 99214 or 99215 is leaving real money on the table, every single day.
A simple quarterly coding audit, reviewing a sample of 20 to 30 claims across your most common code types, can reveal patterns that would otherwise stay invisible. Many practices find that a single round of coding review and education generates measurable revenue improvement within 60 to 90 days.
Patient Collections: The Part of the Revenue Cycle That’s Getting Harder
 High-deductible health plans have shifted a growing portion of the financial responsibility for medical care directly onto patients. In many practices, patient balances now represent 20 to 30% of total revenue, and collecting that money requires a completely different approach than collecting from payers.
High-deductible health plans have shifted a growing portion of the financial responsibility for medical care directly onto patients. In many practices, patient balances now represent 20 to 30% of total revenue, and collecting that money requires a completely different approach than collecting from payers.
The single most effective thing an independent practice can do to improve patient collections is collect at the time of service. Once a patient leaves the building, the probability of collecting their balance drops with every passing week. Providing a cost estimate before or at the visit, and having a clear, comfortable process for collecting copays and known balances at checkout, is the highest-leverage change most independent practices can make to their patient AR.
Point-of-service collection rate is worth tracking separately from your overall collection rate. If you know that you’re collecting 85% of patient balances at the time of service, you have a clear baseline to improve from. If you’ve never measured it, you probably don’t know how much you’re leaving behind.
Payer Mix: The Context That Makes Everything Else Make Sense
Here’s something that often gets overlooked, your revenue cycle benchmarks are only meaningful in the context of your payer mix. A practice with 60% Medicaid volume is going to have different natural AR and collection benchmarks than a practice with 70% commercial insurance. Comparing your numbers to a generic industry average without accounting for payer mix can lead you to conclusions that don’t actually apply to your situation.
Payer mix analysis, which means calculating what percentage of your revenue comes from each payer type, is also one of the most valuable inputs to payer contract strategy. If a specific commercial payer represents 25% of your volume but is consistently slow to pay, high in denials, and reimbursing at rates below your other contracts, that’s a contract worth renegotiating. Without the data, you’d never know which payer to focus on first.
Revenue Cycle Metrics FAQ
- What is a ‘good days’ in AR benchmark for an independent medical practice?
Most specialties should aim for under 35 days. Anything above 50 days typically signals a problem with claim submission speed, eligibility verification, or follow-up workflows. - How do I calculate my net collection rate?
Divide your total payments collected by your total charges minus contractual adjustments, then multiply by 100. Use adjusted charges as your denominator, not gross billed charges, or the number won’t be meaningful. - What is a realistic denial rate target for an independent practice?
The industry benchmark is under 5%. Many independent practices are running at 10 to 15% without realizing it, which represents a significant and recoverable revenue loss. - How often should I review revenue cycle metrics?
Monthly at minimum for the core metrics like days in AR, denial rate, and net collection rate. AR aging should be reviewed monthly as well, with specific attention to claims in the 61-plus day buckets. - When does it make sense to outsource revenue cycle management?
When your internal team is consistently behind on follow-up, your denial rate is above 5%, your days in AR is trending upward, or your net collection rate has dropped below 95%, those are signals that the current approach isn’t keeping up. - Does payer mix affect my revenue cycle benchmarks?
Yes, significantly. A high Medicaid or self-pay volume will naturally affect your collection rate and AR days. Always interpret your metrics in the context of who your patients are and which payers you’re billing.
Summary: Vital Revenue Cycle Metrics for Independent Providers
![]() Revenue cycle metrics aren’t just numbers on a report. They’re a diagnostic tool. When you know your days in AR, your clean claim rate, your denial rate, and your net collection rate, you can see exactly where your practice is losing money and what to do about it. When you don’t know those numbers, you’re making decisions blind.
Revenue cycle metrics aren’t just numbers on a report. They’re a diagnostic tool. When you know your days in AR, your clean claim rate, your denial rate, and your net collection rate, you can see exactly where your practice is losing money and what to do about it. When you don’t know those numbers, you’re making decisions blind.
Independent practices don’t need a finance department to start measuring the right things. They need a clear set of targets, a consistent review process, and the right billing partner to make sure the underlying work is being done accurately and efficiently.
At Medwave, we work with medical practices on billing, credentialing, and payer contracting, and we bring the kind of data-driven approach to revenue cycle management that helps independent practices stop losing revenue they’ve already earned. If you’d like to know how your current metrics stack up and where the biggest opportunities are in your practice, reach out to Medwave. The numbers will tell the story. We’ll help you act on it.
Co-Founder and COO of Medwave, bringing more than 30 years of hands-on experience in healthcare revenue cycle management, payer contracting, and medical credentialing.