

The most common credentialing delays are caused by incomplete applications, mismatched provider data, expired CAQH profiles, incorrect NPI usage, closed payer panels, and communication breakdowns. Each of these is preventable. Yet, only if you know where to look before the application is submitted.
If you work in healthcare administration, you already know the financial stakes. A single delayed application can push a provider’s start date back by months, trigger a wave of claim denials, and put billing teams in damage-control mode. The good news, most of these problems have clear, systematic fixes.
Key Takeaways
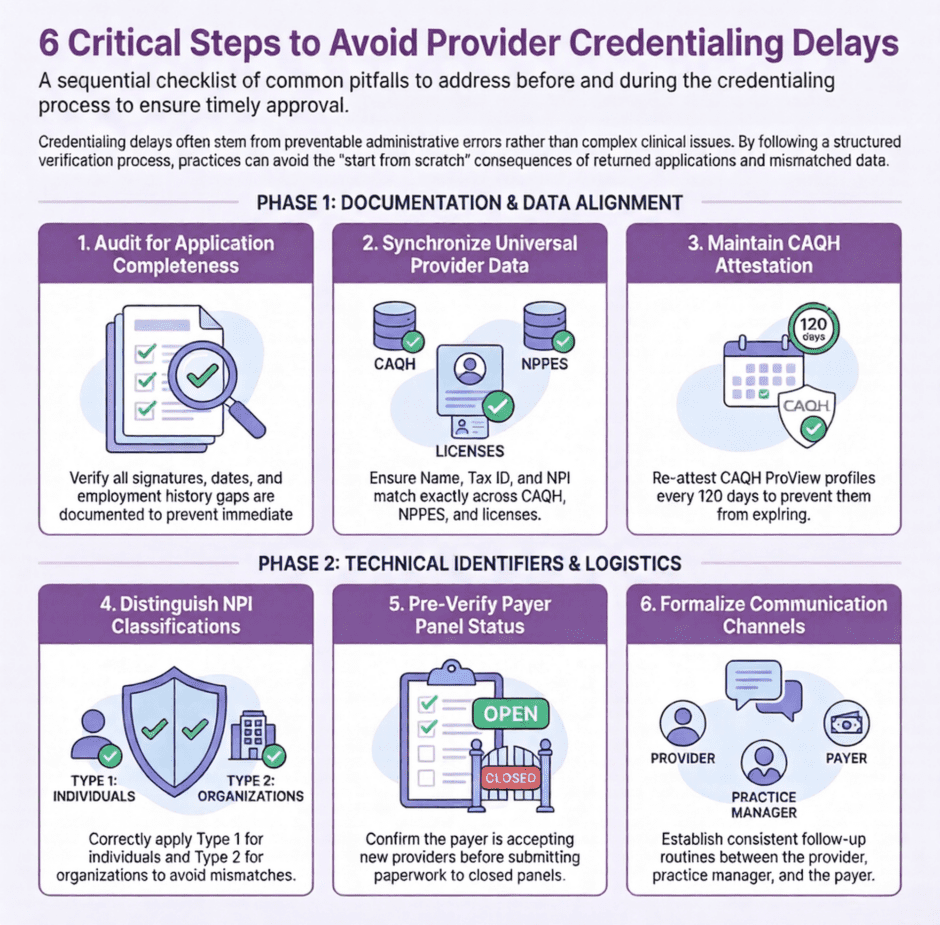
Most credentialing delays are preventable and come down to six root causes:
- Incomplete/inaccurate applications: missing signatures, blank fields, or employment gaps kick the application back and reset your place in queue (adds 2–4 weeks)
- Mismatched provider data: name, DOB, Tax ID, or NPI inconsistencies between the application, CAQH, and NPPES trigger investigations (adds 3–6 weeks)
- CAQH profile problems: expired or incomplete profiles stall every payer relying on CAQH simultaneously; re-attest every 120 days
- Incorrect NPI usage: mixing up Type 1 vs. Type 2 NPIs, or outdated taxonomy codes, routes applications to the wrong department or causes outright rejection
- Closed payer panels: no paperwork fixes this; confirm panel status before submitting to avoid wasting weeks
- Communication breakdowns: slow providers, unresponsive office managers, and inconsistent follow-up all stall the process
Why Credentialing Takes So Long (in the First Place)
Before jumping into what goes wrong, it helps to define things. Credentialing is the formal process by which insurance payers verify a provider’s qualifications, licenses, work history, and professional background before allowing them to participate in a network. Medicare, Medicaid, and commercial payers each have their own requirements, timelines, and systems. What is acceptable for one payer may not fly with another.
On a good day, commercial credentialing typically runs 60 to 120 days with major payers like UnitedHealthcare, Anthem, and Cigna. Medicare enrollment through PECOS averages 60 to 90 days under normal conditions, but can extend to 120+ days when PECOS flags discrepancies or when the MAC (Medicare Administrative Contractor) has processing backlogs. Medicaid timelines vary by state, from as few as 30 days in some states to 120+ days in others. For every week a provider isn’t credentialed, a full-time physician typically represents $3,000–$7,000 in lost or delayed revenue per week, making speed an economic issue, not just an administrative one.
That kind of workload leaves a lot of room for small problems to become big ones.
What are the Most Common Causes of Credentialing Delays?
1. Incomplete or Inaccurate Applications
This is the number one reason applications get kicked back. Missing signatures, blank fields, or outdated references give payers an easy reason to return the application without processing it. Sometimes it is something as simple as a missing date or a signature in the wrong spot. Other times it is a more significant gap, like missing work history or an explanation for a gap in employment.
Every returned application adds weeks to your timeline. The application has to be corrected, resubmitted, and then placed back in the payer’s queue. If the payer has a backlog, you are starting from scratch.
2. Mismatched Provider Data
Provider data has to match across every source a payer checks. That means the name, date of birth, address, Tax ID, and NPI on the application need to align exactly with what is on file at CAQH, the NPPES database, and the provider’s license. One small inconsistency, even something like a middle initial or a street address abbreviation, can hold up an application for weeks while the discrepancy gets investigated.
This is more common than you might think, especially when providers have recently moved, changed their practice setup, or gone through a name change.
3. CAQH Profile Problems
CAQH ProView is the centralized credentialing database that most commercial payers pull from. If a provider’s CAQH profile is incomplete, expired, or not authorized for the right payers, the entire application can be delayed before it ever reaches a payer’s credentialing department. CAQH mistakes hurt providers.
Providers must re-attest their CAQH ProView profiles every 120 days, roughly every four months. Missing this window causes the profile to lapse, and payers querying CAQH will receive stale or incomplete data. An expired CAQH profile doesn’t just slow one application; it holds up every payer that uses CAQH for primary source verification simultaneously. The fix is simple but requires a system. Set a calendar reminder 2 weeks before the 120-day mark so your team can prompt the provider to re-attest before the profile goes stale. CAQH also sends email reminders, but these are easy to miss in a busy inbox. Don’t rely on them as your only trigger.
4. Incorrect NPI Usage
Providers have two types of National Provider Identifiers. A Type 1 NPI belongs to the individual provider. A Type 2 NPI belongs to the organization or group practice. Using the wrong one on an application is a surprisingly common mistake that creates a mismatch payers cannot easily sort out on their own.
Beyond mix-ups, outdated NPPES data is a silent credentialing killer. If a provider’s taxonomy code doesn’t match their current specialty, payers may reject the application outright or route it to the wrong credentialing department. A nurse practitioner who transitioned to psychiatry but still carries a primary care taxonomy code (363L00000X) will run into conflicts with behavioral health payers expecting taxonomy 101YA0400X. Corrections must be made directly at the NPPES website (nppes.cms.hhs.gov), and updates can take 7–14 days to propagate across payer systems, so address this well before submitting applications.
5. Closed Payer Panels
Some payers are not accepting new providers at all. A closed payer panel means the payer has enough in-network providers in a given specialty or geographic area and is not credentialing new ones. This is a situation that no amount of paperwork can fix in the short term.
The problem is that many applicants do not find out a panel is closed until weeks into the process. Getting that information upfront, before submitting, saves time and prevents frustration.
6. Poor Communication with Clients and Representatives
Credentialing does not happen in a vacuum. It requires back-and-forth between the credentialing team, the provider, the practice manager, and the payer’s enrollment or provider relations department. When any of those communication lines break down, delays happen.
Providers who are slow to return requested documents, office managers who do not respond to payer inquiries, and credentialing staff who do not follow up consistently all contribute to stalled applications. It is a team effort, and when one part of the team goes quiet, the whole process can grind to a halt.
How to Prevent Delays Before They Start
Prevention starts at the intake stage. Before any application is submitted, every piece of provider data should be verified and cross-referenced.
Here is a practical checklist for cleaner submissions:
- Confirm the provider’s NPI type and verify NPPES data is current
- Check that the CAQH profile is complete, up to date, and attested within the last 120 days
- Verify that the Tax ID matches the IRS records for the practice entity
- Confirm all licenses are active, with no pending actions or expirations within 90 days
- Check for malpractice coverage that meets payer minimums
- Confirm DEA registration if applicable to the specialty
- Verify provider addresses are consistent across all documents
- Contact the payer to confirm the panel is open before submitting
This kind of front-end verification adds a small amount of time before submission, but it saves a much larger amount of time on the back end. Follow that checklist to prevent credentialing delays.
What Should a Credentialing Tracking System Include?
 One of the biggest gaps in credentialing operations is the lack of a reliable tracking system. When you are managing multiple providers across multiple payers, you need to know exactly where each application stands at all times.
One of the biggest gaps in credentialing operations is the lack of a reliable tracking system. When you are managing multiple providers across multiple payers, you need to know exactly where each application stands at all times.
A good tracking system does not have to be fancy. It needs to capture the submission date, the expected turnaround window for each payer, the date of the last follow-up, and the name of the payer rep you spoke with. It should flag applications that are approaching or exceeding standard payer timelines so you can take action before a delay becomes a denial.
Follow-up calls should be scheduled at regular intervals, typically every 10 to 15 business days for active applications. Document every call, including who you spoke with, what they said, and what the next step is. This documentation is your paper trail if you need to escalate.
When Should You Escalate a Credentialing Delay and How?
Even with a solid tracking system and clean submissions, some applications will still run long. Knowing when to escalate is just as important as knowing how to submit.
Most payers publish standard credentialing timelines. When an application exceeds that window without resolution, it is time to move up the chain. Start with the payer’s provider relations department. If that does not yield results, request a supervisor or formal escalation. For Medicare issues, CMS has a help desk and ombudsman resources available to providers who are experiencing enrollment problems.
When escalating, be specific. Have your application reference numbers, submission dates, and documentation of all prior contacts ready. Vague complaints are easy to dismiss. A clear, documented timeline of what has happened and what you are requesting is much harder to ignore.
How Do You Manage Provider Expectations During Credentialing?
 Providers are not always aware of how long credentialing takes or how much can go wrong along the way. Part of a credentialing professional’s job is setting realistic expectations from the start.
Providers are not always aware of how long credentialing takes or how much can go wrong along the way. Part of a credentialing professional’s job is setting realistic expectations from the start.
At intake, give providers a clear timeline based on the specific payers involved. Explain what you need from them and when you need it. Make it clear that delays on their end, like a slow response to a document request, have a direct impact on when they will be approved. Most providers are cooperative once they grasp the connection between their responsiveness and their revenue.
Regular status updates go a long way toward keeping providers calm and engaged. A quick email every two to three weeks letting them know where things stand takes very little time and prevents a lot of anxious phone calls.
How Do Payer-Specific Requirements Affect Credentialing Timelines?
No two payers credential exactly the same way. Some have online portals. Some require paper applications. Some require primary source verification on top of what CAQH already provides. Some have delegate credentialing agreements that allow credentialing organizations to process applications on their behalf, while others insist on doing everything in-house.
Getting familiar with the specific requirements and quirks of the payers you work with most often is one of the most practical investments a credentialing team can make. Build a reference guide for each payer. Note their current panel status, their typical timeline, their preferred method of contact, and any common sticking points you have encountered. That institutional knowledge pays dividends every time you work with that payer again.
How Long Can a Credentialing Delay Last?
 The duration of a credentialing delay depends on what caused it. A returned application due to a missing signature adds 2–4 weeks while it’s corrected, resubmitted, and placed back in queue. A mismatched data discrepancy that requires investigation can add 3–6 weeks. A closed payer panel has no fixed timeline, panels may reopen in 90 days or not for a year or more.
The duration of a credentialing delay depends on what caused it. A returned application due to a missing signature adds 2–4 weeks while it’s corrected, resubmitted, and placed back in queue. A mismatched data discrepancy that requires investigation can add 3–6 weeks. A closed payer panel has no fixed timeline, panels may reopen in 90 days or not for a year or more.
As a general rule, every returned application resets your position in the payer’s queue. For high-volume payers with monthly credentialing committees, this can mean missing an entire review cycle, adding 30 days per occurrence. Medicare PECOS delays following an error can run 60–90 additional days in worst-case scenarios. This is why front-end verification before submission is worth more than any escalation strategy after the fact.
Delayed Credentialing FAQs
What is the most common reason for a credentialing delay?
The most common reason for credentialing delays is an incomplete or inaccurate application. Missing signatures, blank fields, undated entries, or gaps in work history give payers an automatic reason to return the application, resetting your position in their review queue and adding 2–4 weeks to your timeline.
How long does a credentialing delay typically last?
A single returned application adds 2–4 weeks. A data discrepancy under investigation can add 3–6 weeks. Closed payer panels may delay enrollment for 90 days to over a year. Medicare PECOS errors can extend timelines by 60–90 additional days in worst-case scenarios.
How do I prevent credentialing delays?
Prevent credentialing delays by verifying provider data before submission: confirm NPI type and NPPES accuracy, ensure CAQH is attested within 120 days, check that Tax ID matches IRS records, verify all licenses are active, confirm malpractice coverage meets payer minimums, and call to confirm the payer panel is open.
What happens when a CAQH profile expires?
When a CAQH profile expires, payers querying the database receive stale or incomplete data, which stalls every application relying on that profile simultaneously. Providers must re-attest every 120 days. An expired profile does not automatically invalidate submitted applications, but it significantly delays processing.
Can you bill insurance while credentialing is pending?
In most cases, you cannot bill a payer’s network rates while credentialing is pending. Some payers allow retroactive billing once credentialing is approved, called credentialing back-billing, but this is payer-specific and not guaranteed. Confirm retroactive billing policies with each payer at the time of application.
When should you escalate a credentialing application?
Escalate when an application has exceeded the payer’s published standard timeline without resolution. For most commercial payers, this threshold is 90–120 days. Start with the payer’s provider relations department, then request a supervisor or formal escalation. For Medicare, CMS maintains ombudsman and help desk resources for enrollment delays.
Summary: Fixing Delays in Credentialing
![]() Credentialing is one of those processes where an ounce of prevention genuinely is worth a pound of cure. A clean application submitted to the right payer with verified data and a fully attested CAQH profile will almost always move faster than one that needs to be corrected and resubmitted. Good tracking and consistent follow-up catch problems before they become disasters. Clear communication with providers and payers keeps everyone on the same page.
Credentialing is one of those processes where an ounce of prevention genuinely is worth a pound of cure. A clean application submitted to the right payer with verified data and a fully attested CAQH profile will almost always move faster than one that needs to be corrected and resubmitted. Good tracking and consistent follow-up catch problems before they become disasters. Clear communication with providers and payers keeps everyone on the same page.
None of this requires a perfect system. It requires a disciplined one.
At Medwave, we work with healthcare providers every day on exactly these kinds of challenges. Our team handles medical billing, credentialing, and payer contracting, giving practices the support they need to get in-network faster and keep revenue flowing without interruption. If your credentialing process feels like it is always behind, or if you are tired of chasing payers for answers, we are here to help.
Co-Founder and COO of Medwave, bringing more than 30 years of hands-on experience in healthcare revenue cycle management, payer contracting, and medical credentialing.