
If you’re a healthcare provider trying to get paid by insurance companies, you’ve likely encountered the terms “credentialing” and “contracting” more times than you can count. While these processes are often mentioned together, they serve distinctly different purposes in establishing your ability to treat patients and receive reimbursement from payers.
Many providers assume these terms are interchangeable or think completing one automatically takes care of the other. This misconception can lead to significant delays in getting paid, frustrated patients, and missed revenue opportunities. Getting clarity on these differences isn’t just academic, it directly impacts your practice’s financial health, operational efficiency, and ability to serve patients effectively.
Key Takeaways
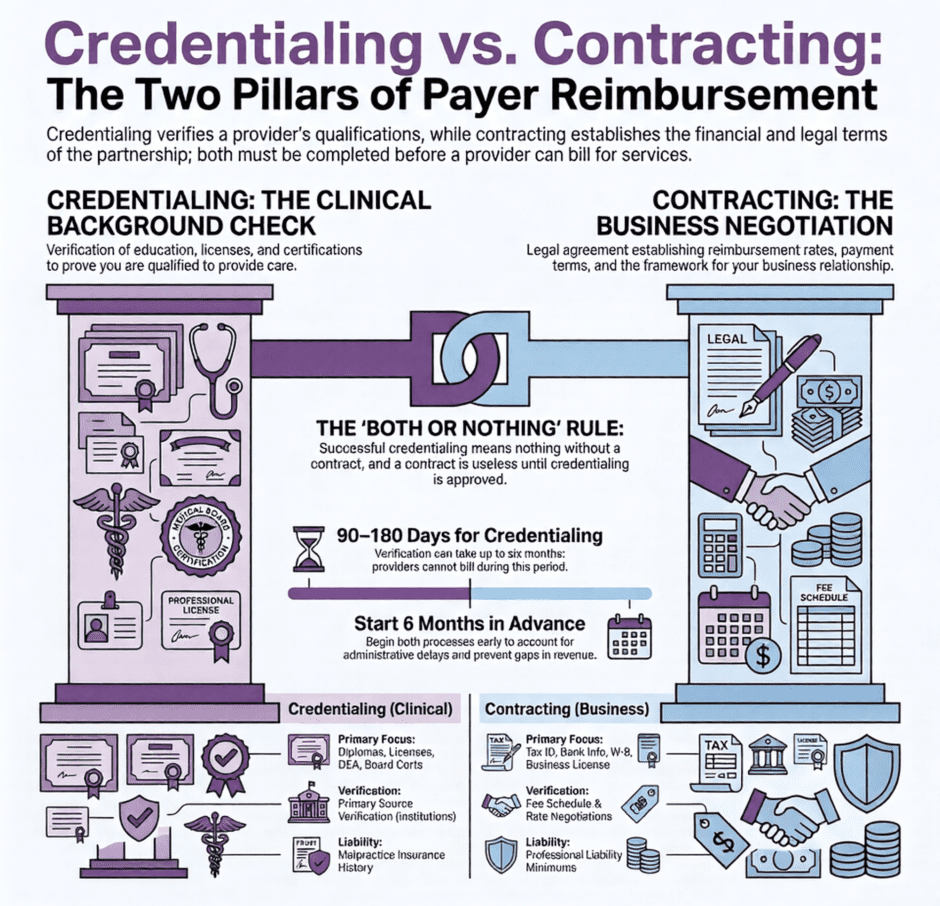
Credentialing verifies a provider’s qualifications; contracting negotiates payment terms. They are separate processes with separate timelines. Credentialing typically takes 90-180 days. You cannot bill a payer during this window, even with a signed contract. Contracting can finalize in as little as 30 days or take several months, depending on negotiation complexity. Most payers require credentialing approval before starting contract negotiations, though some run the two in parallel. Both must be complete before a provider can bill and get paid, combined timelines of six months or more are common for new payer relationships.
What is Credentialing?
Credentialing is the verification process that insurance companies use to evaluate your qualifications, training, and professional background before allowing you to treat their members. During credentialing, payers examine your medical education, residency training, board certifications, state licenses, malpractice insurance, and professional history.
The credentialing process typically takes 90 to 180 days. During this time, you cannot bill the insurance company for services rendered to their members, even if you have a signed contract with them.
Credentialing requirements also vary by payer. Some require site visits, additional documentation for specific specialties, or supplementary training certifications beyond the standard verification checklist, which is another reason two payers with seemingly similar requirements can still land on very different timelines.
What is Contracting?
Contracting is the business negotiation that establishes the terms under which you’ll be paid for treating a payer’s members. This process focuses on financial arrangements, payment rates, covered services, and the legal framework governing your relationship with the insurance company.
Contracting timelines vary; some standard contracts finalize within 30 days, while others take several months if significant negotiation is involved.
Contracting requirements also vary by payer size and structure. Larger payers often work from standardized template agreements with limited room for negotiation, while smaller or regional payers may offer more flexibility on rates and terms, particularly for practices with strong specialty demand or an existing track record with that payer.
Credentialing vs. Contracting: Side-by-Side Comparison
| Factor | Credentialing | Contracting |
|---|---|---|
| Purpose | Verifies provider qualifications and background | Negotiates payment terms and financial arrangements |
| Typical timeline | 90-180 days | 30 days to several months |
| Focus | Education, licensure, board certification, malpractice history | Reimbursement rates, covered services, billing terms |
| Who's evaluated | The individual provider | The practice's business relationship with the payer |
| Required before billing? | Yes, without it claims are denied | Yes, without it there's no agreed payment rate |
| Renewal cycle | Every 2-3 years (recredentialing) | At contract expiration or renegotiation |
| Documents needed | Diplomas, licenses, DEA registration, malpractice insurance | Tax ID, W-9, liability insurance certificates, banking info |
How Do Credentialing and Contracting Work Together?
While credentialing and contracting are separate processes, both must be complete before you can bill a payer for services. A signed contract with attractive rates means nothing if credentialing isn’t finished, and successful credentialing means nothing without a contract that sets your payment rate.
The relationship generally follows this sequence:
- Application submission, you submit credentialing documents and, where allowed, an initial contract request to the payer
- Primary source verification, the payer verifies your education, licensure, and history directly with issuing institutions
- Committee review, a credentialing committee approves or denies your application based on the payer’s standards
- Contract offer, once credentialed, the payer issues contract terms, or finalizes terms negotiated in parallel
- Negotiation and execution, you and the payer agree on rates and terms, then sign
Most payers require credentialing approval before they’ll consider contract negotiations, though some allow the two to run in parallel. Some payers streamline this further with combined applications or coordinated timelines, though this varies widely, large national payers tend to run more standardized processes, while smaller regional payers can carry unique requirements for both credentialing and contracting. Adding a new provider to an existing practice requires fresh credentialing with each payer, but that provider typically operates under the practice’s existing contracts. Contract renewals, by contrast, don’t usually require re-credentialing unless there’s been a material change to provider qualifications or practice structure.
What Regulations Govern Credentialing and Contracting?

Credentialing and contracting sit under different compliance frameworks, and mixing them up can create real exposure.
Credentialing compliance centers on professional standards and patient safety. The Joint Commission, the National Committee for Quality Assurance (NCQA), and CMS all maintain credentialing standards that healthcare organizations must follow, including verification depth and recredentialing frequency.
Contracting compliance involves a different set of rules entirely, including the federal Anti-Kickback Statute and Stark Law provisions governing physician self-referral. Contracts must avoid arrangements that could be read as improper referral incentives, separate from anything related to a provider’s individual qualifications.
Technology reflects this same split. Credentialing platforms are generally built around verification workflows and document management, tracking license expirations and upcoming renewals. Contracting systems instead focus on relationship and performance management, supporting the contract lifecycle from initial negotiation through renewal or termination. Practices managing both often need separate systems, or a partner who can bridge the two without losing visibility on either side.
How Long Do Credentialing and Contracting Take?
Since credentialing alone can take 90 to 180 days, and contracting can add more time on top of that, you could be looking at six months or more before your first reimbursement from a new payer. This timeline carries real operational weight. Many practices maintain detailed tracking systems that monitor the status of credentialing and contracting applications across multiple payers at once, which helps surface delays early and supports better cash flow planning during transition periods.
Plan around this reality:
- Start credentialing well before you plan to see patients under a new payer
- Build in buffer time, payer requirements shift, and additional documentation requests are common
- Track applications across payers so delays surface early rather than at the point of a denied claim
What Documentation Does Each Process Require?
Credentialing documentation proves you’re qualified to practice. This includes medical school diplomas and transcripts, residency and fellowship certificates, current state licenses, DEA registration, board certification, malpractice insurance certificates, and professional references. Some payers add site visits or specialty-specific requirements.
Contracting documentation establishes the business framework. This includes tax identification numbers, business licenses, liability insurance meeting contract minimums, banking information for electronic payments, and completed W-9 forms.
What Are the Most Common Credentialing and Contracting Mistakes?
The most persistent mistake is assuming the two processes are interchangeable, or that finishing one automatically finishes the other. A close second, assuming credentialing with one payer transfers to another. It doesn’t. Every payer runs its own independent process.
Other common mistakes that delay both processes:
- Submitting incomplete applications or missing documentation
- Not responding promptly to requests for additional information
- Letting licenses, certifications, or insurance coverage lapse
- Treating a verbal agreement as a valid contract
- Not tracking application status or following up
These errors are avoidable with basic process discipline, but they remain some of the most common reasons practices see longer-than-expected timelines with a new payer.
How Do Credentialing and Contracting Affect Your Bottom Line?
Credentialing delays mean months of uncompensated care or turned-away patients. Contracting terms directly set your reimbursement rate, and a poorly negotiated contract can suppress your revenue for years.
Poor contract terms carry long-lasting financial consequences of their own. Low reimbursement rates, unfavorable billing terms, or restrictive coverage policies can affect your bottom line for years, while effective negotiation can secure better rates and more favorable payment terms from the start.
Costs on both sides are typically front-loaded, application and verification fees for credentialing, legal review and negotiation time for contracting, and are usually recovered once both processes are complete and billing begins. Many practices maintain a cash reserve or line of credit specifically to cover the gap while new payer relationships are still in process.
What Are the Best Practices for Managing Both Processes?
Regular audits of your credentialing and contracting documentation reduce the risk of delays caused by expired licenses or lapsed insurance coverage, and clear internal ownership keeps applications moving instead of stalling in someone’s inbox.
- Start both processes as early as possible, ideally several months ahead of when you need to bill a given payer
- Maintain organized, digital documentation with expiration tracking
- Assign clear internal ownership for application status and follow-up
- Build standardized checklists for both credentialing and contracting submissions
- Keep backup documentation current for every required credential
Should You Work With a Professional Credentialing and Contracting Service?
Professional services bring established payer relationships and systematic processes that reduce delays and improve contract terms. That includes application preparation, document verification, payer relationship management, and ongoing maintenance of credentials and contracts.
Medwave handles credentialing and payer contracting together, which means credentialing gaps and contract terms are managed with visibility into how they affect your actual claims and revenue, not as three disconnected functions.
When evaluating a service, look at their experience with your specific payer mix, track record on processing time, fee structure, and ongoing support. The decision often comes down to a straightforward cost-benefit comparison, professional services carry fees, but the time saved, improved contract terms, and reduced administrative burden frequently justify the expense, particularly for practices expanding into new payer networks or growing across multiple locations at once.
FAQ
Can I bill a patient’s insurance if I’m contracted but not yet credentialed?
No. Credentialing must be complete before you can submit claims to a payer, even if a signed contract is already in place.
Does being credentialed with one payer help me get credentialed with another?
No. Each payer runs its own independent credentialing process, even when the requirements look similar on the surface.
Do I need to redo credentialing every time I sign a new contract with the same payer?
Not usually. Contract renewals don’t typically trigger re-credentialing unless there’s been a significant change to your qualifications or practice structure.
How much does credentialing and contracting cost?
Credentialing costs include application and verification fees; contracting costs typically involve legal review and negotiation time. Both are generally offset by the revenue gained once you’re active with a payer.
Can credentialing and contracting happen at the same time?
Some payers allow this, but most require credentialing approval before they’ll begin contract negotiations.
What comes first, credentialing or contracting?
In most cases, credentialing comes first since payers generally require verified provider qualifications before opening contract negotiations.
Is credentialing the same as payer enrollment?
No. Credentialing verifies qualifications; enrollment is the administrative step of being added to a payer’s system to bill. A provider can be credentialed but not yet enrolled.
What happens if a provider bills before credentialing is finished?
Claims are denied. Common denial codes tied to credentialing gaps include CO-97 and CO-4.
How long until a new provider can start generating revenue from a new payer?
Often six months or more once combined credentialing and contracting timelines are factored in.
Summary: Credentialing vs. Contracting
![]()
Credentialing and contracting are distinct but interconnected processes, and getting both right the first time protects your revenue timeline. Neither can be rushed, and both need ongoing maintenance to stay compliant and keep terms favorable. Treating them as a single blended task is one of the most common reasons practices underestimate how long it takes to start generating revenue from a new payer.
Medwave supports practices across all three core functions, billing, credentialing, and payer contracting, so nothing falls through the cracks between verification, negotiation, and getting claims paid. Contact us to help with any credentialing, contracting, or billing needs your practice is facing.
Co-Founder and COO of Medwave, bringing more than 30 years of hands-on experience in healthcare revenue cycle management, payer contracting, and medical credentialing.