
A new physician joins a practice in January, starts seeing patients immediately, and claims go out. Payments come in for several weeks. Then in April the practice receives a letter from a major payer demanding repayment on three months of claims. The reason, the provider was not fully credentialed when those services were billed.
Retroactive recoupment from credentialing gaps happens regularly in medical practices. The gap often goes undetected for weeks or months because some claims slip through payer systems before the credentialing deficiency is flagged, giving the practice a false sense that billing is processing correctly.
This article covers what happens to claims when a provider is not credentialed with a payer, the financial and compliance consequences, and the specific steps that prevent and resolve credentialing gaps.
Key Takeaways
Seeing patients without active payer credentialing means denied claims, possible recoupment of money already paid, compliance exposure, and frustrated patients. Most credentialing gaps are preventable. The ones that aren’t are fixable, but only if you act fast.

Credentialed, Enrolled, and In-Network are Not the Same Thing
Before getting into the consequences, it helps to be clear on terminology, because these three terms get used interchangeably when they shouldn’t.
Credentialing
Credentialing is the process of verifying a provider’s qualifications. Their license, education, training, malpractice history, and certifications. It’s the insurance company or facility confirming that the provider is who they say they are and is qualified to provide the services they’re billing for.
Enrollment
Enrollment is what happens after credentialing. Once a provider is verified, payer enrollment adds them to the payer’s system so claims can be processed under their NPI. Without enrollment, even a fully credentialed provider can’t get paid.
Getting In-Network
In-network means the provider has an active contract with that payer at negotiated rates. You can be enrolled without being in-network, and the difference affects what patients owe.
When people talk about a “credentialing gap,” they usually mean a provider who is seeing patients and submitting claims before this entire chain is complete. Sometimes credentialing is done but enrollment isn’t finished. Sometimes everything lapses because a license expired and nobody caught it. Either way, the result is the same.
What Happens to Claims
 Claims submitted under a provider who is not credentialed or enrolled with the payer are denied.
Claims submitted under a provider who is not credentialed or enrolled with the payer are denied.
When a claim is submitted for a provider who isn’t credentialed or enrolled with that payer, the payer’s system flags it and returns it with a denial code. Common credentialing-related denial codes include CO-97 (the benefit for this service is included in the payment/allowance for another service), CO-4 (the service is inconsistent with the modifier), and PR-96 (non-covered charge). The specific code varies by payer, but the result is the same, no payment.
The frustrating part is that some claims don’t get denied right away. Payers don’t always catch credentialing issues on the first pass. A claim slips through, gets paid, and the practice moves on assuming everything is fine. Then the payer runs an audit, discovers the provider wasn’t properly enrolled during that period, and sends a recoupment letter.
Retroactive recoupment is exactly what it sounds like. The payer wants money back, sometimes with interest, sometimes covering several months of claims all at once. For a small practice, a recoupment demand can be a serious financial hit.
The Financial Consequences are Bigger Than One Denied Claim
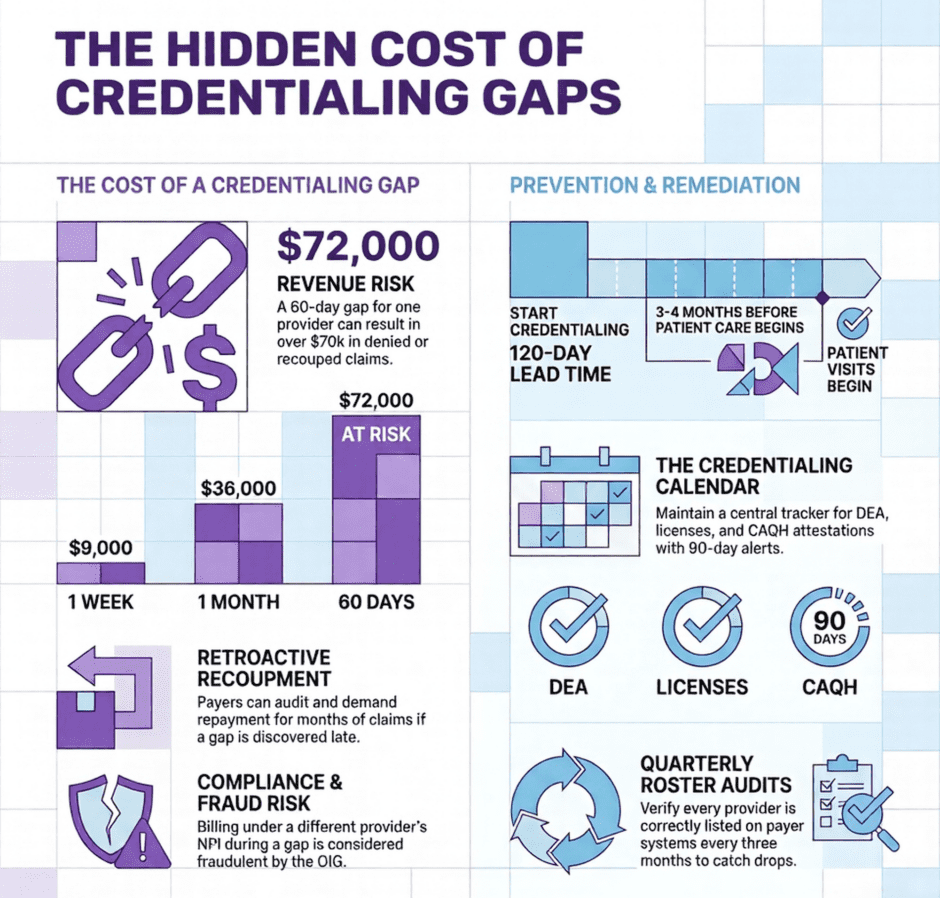
A provider seeing 15 patients per day at an average reimbursement of $120 per claim generates approximately $9,000 per week in billings. A 60-day credentialing gap represents roughly $72,000 in claims, all of which are either denied on first submission or subject to retroactive recoupment when the payer discovers the gap on audit.
The financial damage doesn’t stop at the denied claims themselves.
The financial damage extends beyond the denied claims themselves. Rework costs accumulate as billing staff review each denial, determine whether an appeal is viable, gather supporting documentation, and resubmit. Most payers allow 90 to 180 days from the date of service to submit a corrected claim. Any claims that age past that window cannot be resubmitted regardless of the circumstances and must be written off. If the credentialing gap spans several months, a portion of that revenue is permanently unrecoverable.
Compliance Risk is Real
 This is the part that tends to get glossed over. Credentialing gaps aren’t just a billing problem. They carry compliance exposure.
This is the part that tends to get glossed over. Credentialing gaps aren’t just a billing problem. They carry compliance exposure.
The most common mistake practices make when facing a credentialing delay is billing under a supervising physician’s NPI. The assumption is that this is a safe workaround. In most cases, it isn’t. Incident-to billing has specific requirements under Medicare, and using another provider’s NPI for services they didn’t supervise or perform is considered fraudulent billing under the False Claims Act.
The OIG takes this seriously. Investigations triggered by billing patterns, whistleblower complaints, or payer audits have resulted in significant penalties for practices that billed under the wrong NPI during a credentialing gap. “We didn’t know the rules” is not a defense that tends to go well.
State regulations add another layer. Several states have their own false claims statutes that operate independently of the federal rules, meaning the liability can stack. The compliance risk alone is reason enough to treat credentialing maintenance as a priority, not an afterthought.
Patients Get Caught in the Middle
Providers sometimes underestimate how credentialing problems affect patients. When a provider isn’t credentialed with a patient’s insurance, the patient may be billed as though they saw an out-of-network provider, even if they specifically chose that provider because they appeared in-network.
That means higher out-of-pocket costs, surprise bills, and in some cases, collections activity on amounts the patient never expected to owe. These situations generate complaints, damage the practice’s reputation, and sometimes result in state insurance department complaints that attract additional scrutiny.
Patient trust is hard to rebuild after a billing surprise like that. And in a small practice where referrals and word-of-mouth drive a meaningful share of new patients, the reputational cost matters.
Why Credentialing Gaps Happen
 Most gaps are preventable. They tend to fall into a handful of recurring patterns.
Most gaps are preventable. They tend to fall into a handful of recurring patterns.
The most common is the new provider problem. A physician or APP joins the practice and starts seeing patients before credentialing is complete. The pressure to generate revenue is real, but starting to bill too early creates exactly the problem you’re trying to avoid.
The second most common is lapsed credentials. A provider’s medical license, DEA registration, board certification, or malpractice coverage expires. The payer’s credentialing file becomes outdated, which can trigger a retroactive gap in coverage with some carriers.
A few other causes worth knowing:
- CAQH profile lapses. CAQH ProView requires attestation every 120 days. A lapsed profile can stall re-credentialing with every commercial payer that uses CAQH simultaneously.
- Practice changes not reported. Moving to a new address, changing your group NPI, or adding a new practice location all require payer notification. Failing to report these changes can disrupt active credentialing.
- Telehealth expansion. Providers who started seeing patients in new states during the telehealth expansion often didn’t obtain the corresponding payer credentials for those states. That gap is still catching practices off guard.
What to Do If You’ve Found a Gap
Finding out your practice has a credentialing gap is stressful. Here’s a practical sequence to follow.
Start with a full audit. Pull a list of every active provider, then cross-reference it against your credentialing records for every payer you bill. Identify which providers are fully enrolled, which are pending, and which have expired or lapsed credentials.
Contact your payers directly. Some payers will consider a retroactive effective date if the credentialing gap was caused by processing delays on their end and you can document the application timeline. This doesn’t always work, but it’s worth the conversation.
File appeals on denied claims with documentation showing the credentialing timeline, when the application was submitted, when it was approved, and why the gap occurred. A well-documented appeal with a clear explanation of the timeline gives you the best chance of recovering denied amounts.
Prioritize by volume. Focus first on the payers that represent the highest share of your claims and the providers generating the most revenue. Trying to fix everything simultaneously usually means nothing gets done well.
Finally, document every step you take. If the situation ever escalates to an audit or a compliance review, a documented remediation effort demonstrates good faith.
How to Prevent This From Happening Again
 Prevention is a lot cheaper than remediation.
Prevention is a lot cheaper than remediation.
Build a credentialing calendar that tracks every expiration date for every provider, licenses, DEA registrations, malpractice policies, board certifications, and CAQH attestation deadlines. Set alerts at 90 days and 30 days before each expiration. Many practices get into trouble simply because nobody owns this tracking responsibility clearly.
Start the credentialing process for new providers the moment you make a hiring decision. Budget 90 to 120 days before they see their first insured patient. If that timeline isn’t practical, use the time productively, new providers can often see self-pay patients or be supervised under appropriate incident-to arrangements while credentialing is pending, as long as the billing is handled correctly.
Do a quarterly audit of your payer rosters. Confirm that every active provider is correctly listed with every payer you bill. Payers occasionally drop providers from their systems without notice, and catching that early is far less painful than discovering it during a denial wave.
‘When You’re Not Credentialed’ FAQ
Can a provider see patients while waiting for credentialing to be approved?
Yes, but billing for those services is the problem. A provider can clinically see patients during a credentialing gap, but submitting claims to the payer before enrollment is complete will result in denials or recoupment. Some practices use self-pay arrangements or incident-to billing during the waiting period, but both require careful handling.
What is the difference between an uncredentialed provider and an out-of-network provider?
An out-of-network provider is credentialed and enrolled with a payer but has no contracted rate agreement. An uncredentialed provider hasn’t completed the enrollment process at all. Out-of-network status results in higher patient cost-sharing. No credentialing at all results in claim denials.
Will a payer backdate credentialing if there was a processing delay on their end?
Some will, with documentation. If you submitted a complete application on time and the payer’s own processing timeline caused the delay, many payers will consider a retroactive effective date. Keep records of every application submission date and all follow-up correspondence.
Can a credentialing gap lead to exclusion from a payer network?
In most cases, a gap alone won’t result in termination from a network. But repeated compliance problems, billing under incorrect NPIs, or a pattern of billing during gaps can attract scrutiny that leads to network review or termination.
How do I know if all my providers are fully credentialed with every payer?
Run a credentialing audit. Pull ERA and EOB data to identify denial codes related to credentialing or enrollment, then cross-reference with your credentialing records. If you don’t have the internal capacity to do this reliably, a billing and credentialing service can do it for you.
What happens if you bill insurance without being credentialed?
Claims will be denied, previously paid claims may be recouped, and depending on how the billing was handled, there may be compliance exposure under state or federal false claims statutes.
How long does it take to get credentialed with a new payer?
Commercial payers typically take 90 to 120 days. Medicare averages 60 to 90 days for a clean application. Medicaid timelines vary by state and can run significantly longer.
Can credentialing be done retroactively?
Some payers will consider a retroactive effective date when delays were caused by their own processing backlogs and the provider can document a timely application. It is not guaranteed, and it varies by payer.
What is a credentialing audit?
A credentialing audit is a systematic review of every active provider’s enrollment status across all payers the practice bills. It identifies gaps, expired credentials, and providers who may be listed incorrectly or not at all on payer rosters.
Summary: When a Provider is Not Credentialed
![]() Credentialing gaps are one of the most avoidable revenue problems in medical practice management. They happen when tracking systems are loose, when new providers start too early, or when nobody owns the ongoing maintenance work. The fixes are not complicated, but they require consistent attention.
Credentialing gaps are one of the most avoidable revenue problems in medical practice management. They happen when tracking systems are loose, when new providers start too early, or when nobody owns the ongoing maintenance work. The fixes are not complicated, but they require consistent attention.
At Medwave, we work with practices on medical billing, credentialing, and payer contracting. That combination matters because credentialing problems show up as billing problems, and billing problems are often connected to how payer contracts are structured. Seeing all three together means we catch things that get missed when those functions are handled separately.
If you’re not certain every provider in your practice is fully enrolled and credentialed with every payer you bill, that’s worth verifying before the next denial wave or recoupment letter shows up. Reach out to us, we’ll help you figure out the gaps.
Co-Founder and COO of Medwave, bringing more than 30 years of hands-on experience in healthcare revenue cycle management, payer contracting, and medical credentialing.