
Most healthcare AI pilots fail not because the technology is flawed but because the data feeding it is fragmented, inconsistent, or structured in ways the AI cannot reliably use. Predictive analytics tools trained on inconsistently coded claims produce unreliable predictions. Prior authorization AI that pulls from incomplete patient records misses critical clinical context. Coding assistants that perform well at one facility underperform at another because the source data looks different.
The underlying problem is data readiness, and it is more widespread than most organizations realize when they start an AI initiative.
Key Takeaways
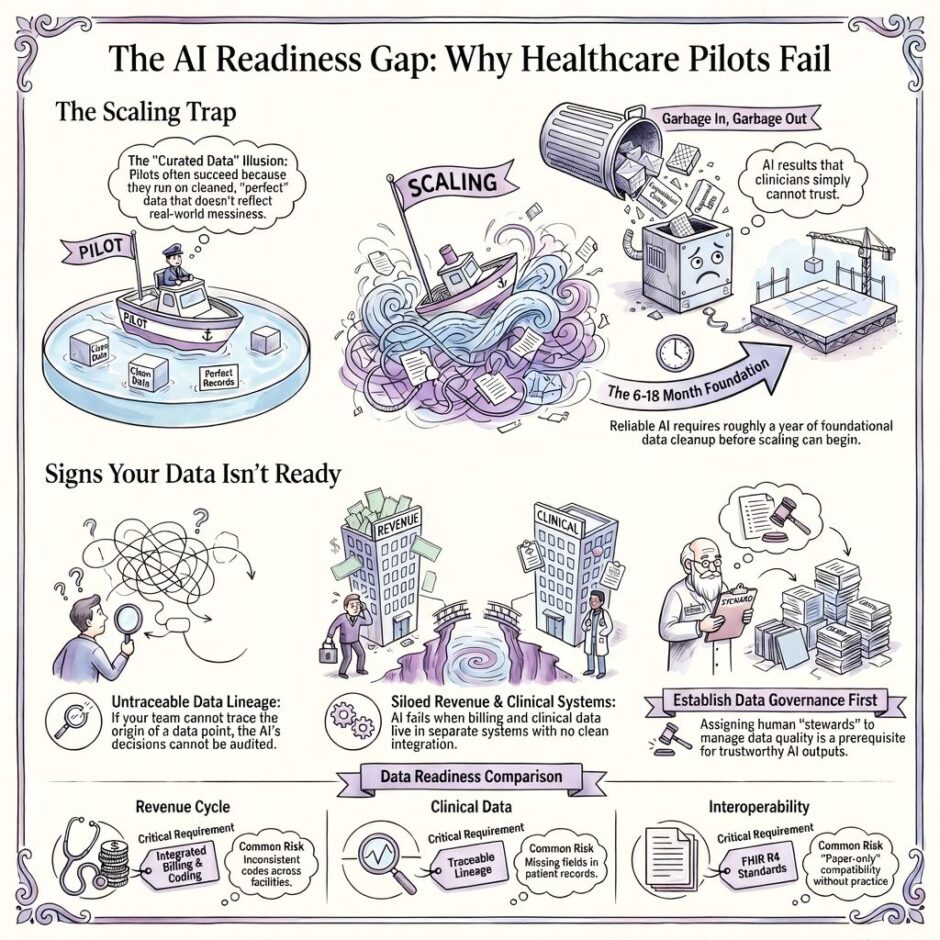
- Most healthcare AI pilots fail at scale because they were tested on curated data that doesn’t reflect the full dataset.
- Fragmented EHR systems, inconsistent coding conventions, and interoperability gaps in practice rather than just on paper are the root causes.
- Weak data governance makes AI outputs unreliable before the tool is even deployed.
- Five specific warning signs indicate whether a healthcare organization’s data is ready for AI at scale.
- Fixing data readiness is a prerequisite for AI that produces trustworthy outputs, not a parallel workstream.
The AI Bottleneck Nobody is Talking About
Healthcare organizations are spending serious money on artificial intelligence right now. Predictive analytics, clinical decision support, automated prior authorization, AI-assisted coding, the use cases are growing fast, and so is the pressure to adopt. But there’s a problem that keeps getting skipped over in vendor demos and executive briefings.
The data isn’t ready. That’s not a minor technical issue.
That might sound like a minor technical issue. It isn’t. When the underlying data feeding an AI system is fragmented, inconsistent, or poorly governed, the AI produces outputs you can’t trust. In healthcare, outputs you can’t trust put patients and revenue at risk.
The question for healthcare organizations in 2026 is not whether to adopt AI. It is whether the data infrastructure can support what the AI is being asked to do.
Why Healthcare Data Can Be So Hard to Use
 Healthcare data is some of the most complicated data in any industry. It comes from dozens of sources, EHRs, billing systems, labs, imaging platforms, pharmacy systems, scheduling tools and very rarely do those sources communicate cleanly with one another.
Healthcare data is some of the most complicated data in any industry. It comes from dozens of sources, EHRs, billing systems, labs, imaging platforms, pharmacy systems, scheduling tools and very rarely do those sources communicate cleanly with one another.
Most health systems are running on multiple EHR platforms, often the result of years of mergers and acquisitions. Each platform records data a little differently. Coding conventions, field names, patient identifiers, these things don’t always line up when you try to bring data together for analysis. Add in the fact that billing and clinical data are often managed by completely separate teams using completely separate systems, and you start to see how fragmented the picture really is.
Interoperability has been a stated goal in healthcare IT for over two decades. Standards like HL7 and FHIR have made real progress, but implementation is inconsistent. Many organizations have interoperability on paper, they can technically exchange data between systems, but the data that comes through is incomplete, out of date, or structured differently than expected. That’s interoperability in theory, not in practice.
Then there’s the data quality problem, which tends to compound quietly over time. Missing fields. Duplicate patient records. Inconsistent use of ICD and CPT codes across facilities and specialties. Billing data recorded one way at an outpatient clinic and a completely different way at a hospital-based department. These aren’t edge cases. They’re routine.
How Bad Data Derails AI
There’s an old saying in data science. Garbage in, garbage out. In healthcare, the stakes attached to that phrase are much higher than in most fields.
When an AI model is trained on or fed data that has quality problems, the outputs reflect those problems. A denial prediction tool trained on inconsistently coded claims will produce unreliable predictions. A prior authorization AI that pulls from incomplete patient records will miss critical clinical context. A coding assistant that works well at one facility may perform poorly at another because the source data looks different.
This is also why so many AI pilots in healthcare look promising early on and then fall apart at scale.
Pilot programs typically run on curated datasets, a controlled slice of your data that has been cleaned up and standardized for the purpose of the test. When the pilot goes live across the full organization, it encounters the real data. All of it. With all its inconsistencies. And suddenly the results aren’t what anyone expected.
This pattern has played out at health systems across the country. Clinicians start questioning the AI’s recommendations. Administrators lose confidence in the outputs. The technology gets shelved or quietly deprioritized, and the organization moves on to the next pilot, without ever fixing the root cause.
Five Signs Your Data is Not AI-Ready
Before your organization commits more resources to AI, it’s worth doing an honest self-assessment.
Five specific patterns indicate that a healthcare organization’s data infrastructure is not ready to support AI at scale:
- You can’t trace where a data point came from. If your team can’t look at an AI output and answer the question “where did this data originate?”, you don’t have data lineage. Without lineage, you can’t audit AI decisions, explain them to clinicians, or trust them in high-stakes situations.
- Your AI results vary significantly by site, specialty, or payer. Inconsistency across business units is almost always a sign that the source data looks different from one place to the next. That’s a data problem, not an AI problem.
- Your team spends more time cleaning data than analyzing it. If data preparation is consuming the majority of your analytics team’s time, your pipelines aren’t reliable. Reliable pipelines are a prerequisite for AI, not a nice-to-have.
- You have no formal data governance policy. If nobody owns data quality, if there are no defined stewards, no quality thresholds, no accountability, AI will inherit whatever state your data happens to be in. That’s a recipe for unreliable outputs.
- Your revenue cycle and clinical data live in completely separate systems with no clean integration. This is one of the most common and costly data gaps in healthcare. Any AI use case that touches billing, prior authorization, or care coordination depends on both data sources working together.
Building a Data Foundation That Can Support AI
 Getting your data AI-ready isn’t a one-weekend project. For most health systems, it’s a 6-to-18-month effort that requires investment, leadership buy-in, and a willingness to prioritize infrastructure over shiny tools. But it’s also the only path to AI that works reliably, at scale, over time.
Getting your data AI-ready isn’t a one-weekend project. For most health systems, it’s a 6-to-18-month effort that requires investment, leadership buy-in, and a willingness to prioritize infrastructure over shiny tools. But it’s also the only path to AI that works reliably, at scale, over time.
Start with a data audit. Before you can fix anything, you need to know what you’re working with. That means inventorying every significant data source in the organization, EHR, billing, credentialing, payer contracts, scheduling, labs, and honestly assessing the state of each one. Which sources are structured? Which are reliable? Which have known quality issues? This audit becomes the foundation for everything else.
Establish data governance before you scale AI. Governance gets treated like a bureaucratic exercise, but it’s actually the thing that makes AI trustworthy. Assign data stewards to each major domain, someone in clinical informatics owns clinical data quality, someone in revenue cycle owns billing data quality, and so on. Define what “good data” looks like in your organization and create processes for catching and correcting data that falls below that standard.
Invest in your data pipelines, not just your AI tools. This is the part that doesn’t show up in vendor pitches. The pipelines that move data from source systems into analytics platforms and AI tools are where a lot of the failure happens. Unreliable ETL processes, batch refresh delays, and API inconsistencies can all introduce errors before the AI ever sees the data. Fixing the pipes is unglamorous work, but it matters enormously.
Make interoperability a vendor requirement. Any new platform you evaluate, whether it’s an AI tool, a billing system, or a credentialing solution, should support FHIR R4 at minimum. More importantly, ask vendors to walk you through what data integration actually looks like 90 days after go-live, not in the demo environment. That’s where the real picture emerges.
The Revenue Cycle Is One of the Highest-Risk Domains
If your organization is using AI to improve revenue cycle performance, denial prevention, coding accuracy, prior authorization, contract optimization, you need to pay especially close attention to the quality of your billing and coding data. This is one of the messiest data environments in healthcare, and it’s also one of the most consequential.
Claims data is often coded inconsistently across facilities and departments. Payer contract terms vary widely and are frequently updated, meaning the data used to model expected reimbursement can go stale quickly. Credentialing records are sometimes siloed from billing workflows, which creates gaps when providers aren’t fully enrolled with a payer but are still seeing patients.
AI tools built on top of this kind of data will produce results that reflect the messiness. Denial prediction models trained on inconsistently coded claims will miss patterns. Contract optimization tools that can’t accurately read payer fee schedules can’t make reliable recommendations. The AI isn’t broken. The foundation is.
Revenue cycle leaders who want AI to work need to treat their billing data, credentialing data, and payer contract data as a unified domain, one that requires its own governance, its own quality standards, and its own stewardship.
What Becomes Possible When the Data Is Right
 It’s worth pausing on why this work matters beyond just making AI function properly.
It’s worth pausing on why this work matters beyond just making AI function properly.
When healthcare organizations build a strong data foundation, the benefits go well beyond AI performance. Clinical decision-making improves because the data clinicians are working from is accurate and complete. Revenue cycle performance improves because billing, credentialing, and payer data are clean, current, and connected. Operational reporting becomes more reliable. And when AI is eventually layered on top of that foundation, it works the way it was supposed to work, consistently, at scale, in a way that clinicians and administrators actually trust.
That’s the version of healthcare AI that changes outcomes. Not the pilot. Not the demo. The version that runs on data you can stand behind.
Healthcare Data (in AI) FAQ
What does “data readiness” mean in the context of healthcare AI?
Data readiness means your organization’s data is accurate, accessible, consistently structured, and governed well enough to produce reliable AI outputs across your entire operation, not just in a controlled test environment. It includes data quality, pipeline reliability, interoperability, and governance.
How long does it take to get healthcare data AI-ready?
It depends on the size of the organization and the current state of your data infrastructure. Most health systems should plan for 6 to 18 months of foundational work before AI can scale reliably. Smaller organizations with more consolidated systems may move faster.
Can AI tools help fix bad data, or does the data need to be clean first?
Some AI tools can assist with data normalization and deduplication, but they work best on data that is already structured and consistently formatted. AI is not a substitute for governance or pipeline reliability. Think of it as a finishing tool, not a foundation builder.
What data domains matter most for healthcare AI to work?
Clinical documentation, billing and coding records, credentialing data, payer contracts, and scheduling information are among the most important, and the most commonly problematic. For any AI use case touching revenue cycle, all three of those domains need to be clean and integrated.
What’s the difference between interoperability and data quality?
Interoperability is about whether systems can share data with one another. Data quality is about whether the data being shared is accurate, complete, and consistently structured. You need both for AI to work well. A lot of organizations have one without the other.
Why do healthcare AI pilots seem to work but then fail when rolled out more broadly?
Pilots usually run on curated, cleaned datasets that don’t reflect the full messiness of your production data environment. When you scale, the AI encounters all the inconsistencies that were screened out during testing. Fixing this requires building a data foundation that is consistent across the organization, not just within a controlled subset.
Is data governance really necessary if we already have an IT team managing our systems?
IT manages system performance and infrastructure. Data governance is about the accuracy, ownership, and quality of the data itself. Those are related but distinct responsibilities. Without formal governance, data quality degrades over time because nobody is accountable for catching and correcting errors before they spread through your systems and into AI outputs.
How should we prioritize data readiness work if we have limited resources?
Start with the data domains most directly tied to your highest-priority AI use cases. If your primary focus is revenue cycle AI, audit your billing, credentialing, and payer contract data first. If clinical decision support is the priority, start with clinical documentation and lab data. Trying to fix everything at once usually means fixing nothing well.
Do smaller healthcare organizations need to worry about data readiness the same way large health systems do?
Yes, but the scope is different. Smaller organizations often have fewer systems to integrate, which can work in their favor. But they also tend to have fewer dedicated data resources, which means quality problems can go undetected longer. The risk is the same regardless of size, AI built on bad data produces bad results.
Summary: Healthcare Organization Data + AI
![]() The healthcare organizations that get the most out of AI won’t necessarily be the ones that adopted it earliest. They’ll be the ones that built the right foundation first. That means cleaning up data, closing interoperability gaps, establishing governance, and treating data infrastructure as a strategic asset rather than an IT afterthought.
The healthcare organizations that get the most out of AI won’t necessarily be the ones that adopted it earliest. They’ll be the ones that built the right foundation first. That means cleaning up data, closing interoperability gaps, establishing governance, and treating data infrastructure as a strategic asset rather than an IT afterthought.
At Medwave, we work with healthcare providers across the country to build and maintain the operational backbone that revenue cycle performance depends on. Our services cover medical billing, provider credentialing, and payer contracting, three data domains that are central to any AI initiative touching the revenue cycle. Clean, current, well-governed data in these areas doesn’t just improve AI performance. It improves everything downstream.
If you’re thinking about AI adoption and wondering whether your revenue cycle data is ready to support it, we’d be glad to help you figure that out. Reach out to the Medwave team and let’s talk about where your data stands and what it would take to get it where it needs to be.
Co-Founder and COO of Medwave, bringing more than 30 years of hands-on experience in healthcare revenue cycle management, payer contracting, and medical credentialing.