If your billing team has ever stared at a denied claim stamped with “credentialing issue” and wondered where to even start, you are not alone. These denials are among the most frustrating in the revenue cycle, partly because they sit at the intersection of two departments that do not always talk to each other as often as they should. Credentialing teams manage provider enrollment. Billing teams manage claims. When something falls between those two functions, claims get denied, revenue gets delayed, and everyone points fingers in a different direction.
This guide is written for clinicians, billing staff, and revenue cycle teams who want a clearer, more practical way to handle credentialing-related claim issues. The goal is to help you tell the difference between a true credentialing problem and a billing or registration error that just looks like one, and to give you a structured process for resolving these issues faster, with less frustration and better cross-department collaboration.
Why Credentialing and the Revenue Cycle Must Work Together
 Credentialing is not just an administrative formality. It is the foundation that makes billing possible. When a provider is not properly credentialed and enrolled with a payer, that payer will not reimburse for services, regardless of how accurate the claim is. The clinical work gets done, the claim goes out, and nothing comes back except a denial.
Credentialing is not just an administrative formality. It is the foundation that makes billing possible. When a provider is not properly credentialed and enrolled with a payer, that payer will not reimburse for services, regardless of how accurate the claim is. The clinical work gets done, the claim goes out, and nothing comes back except a denial.
What makes this particularly frustrating is that credentialing problems are often invisible until a claim fails. A provider may believe they are enrolled with a plan, the billing team may believe everything is in order, and it is only when payment does not arrive that anyone discovers there is a gap. By that point, timely filing windows may be closing, and the revenue recovery process becomes more difficult.
The relationship between credentialing and the revenue cycle is direct and financial. Delays in credentialing mean delays in billing. Errors in enrollment mean denials on claims. And when the two departments operate in isolation rather than in coordination, those problems take longer to catch and longer to fix. Bringing these two functions closer together, through shared information, clear communication, and defined processes, is one of the most practical things a practice can do to protect its revenue.
Credentialing vs. Enrollment vs. Billing: Knowing the Difference
Before you can fix a problem, you need to know what kind of problem you are actually dealing with. These three terms get used interchangeably in many practices, but they refer to distinct processes, and mixing them up leads to misdirected troubleshooting.
- Credentialing is the process of verifying a provider’s qualifications. It confirms licensure, education, training, work history, malpractice history, and board certifications. This is primarily a quality and compliance function. Hospitals and payers conduct credentialing to verify that a provider meets their standards before granting privileges or network participation.
- Enrollment, sometimes called payer enrollment or provider enrollment, is the administrative process of registering a provider with an insurance company so they can bill and receive reimbursement. A provider can be credentialed but not yet enrolled, which means they have been verified as qualified but have not yet completed the steps required to bill that specific payer. This distinction matters because it is often the source of confusion when a claim is denied.
- Billing is the process of submitting claims to payers for reimbursement. Billing errors, which include incorrect codes, wrong rendering provider information, or missing modifiers, can cause denials that look like credentialing problems on the surface but are not. A claim that fails because the billing team used the wrong NPI, for example, is a billing error. A claim that fails because the provider was never enrolled is an enrollment problem. Treating them the same way wastes time and delays resolution.
Understanding which category a problem falls into is the first step in fixing it efficiently.
The Most Common “Credentialing” Issues
Not every denial labeled as a credentialing issue is actually a credentialing issue. In practice, these denials tend to fall into a handful of categories, and knowing what to look for saves significant time.
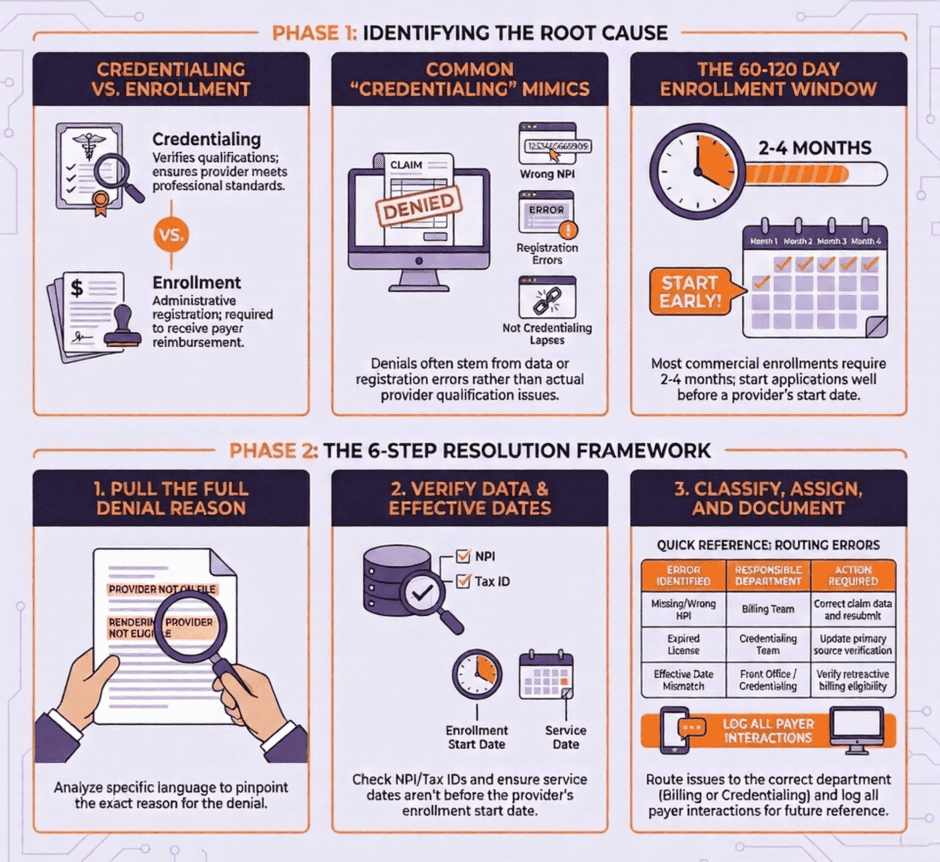
- Provider not yet enrolled with the payer. This is the most straightforward version of a true credentialing-related denial. The provider has been credentialed, meaning their qualifications have been verified, but the enrollment application has not been completed or approved. Claims submitted before enrollment is active will be denied. The fix is to confirm enrollment status directly with the payer and hold claims until approval is received, or explore whether the payer allows retroactive billing once enrollment is active.
- Wrong NPI on the claim. Providers have both an individual NPI (Type 1) and potentially a group NPI (Type 2). Payers have specific requirements about which NPI should appear in which field on the claim. Submitting the individual NPI when the payer expects the group NPI, or vice versa, will generate a denial that may appear to be a credentialing issue but is actually a billing setup error.
- Provider enrolled under a different group or tax ID. If a provider has been enrolled with a payer under a previous employer’s group or tax ID, and has since moved to a new practice, their enrollment at the new practice has to be established separately. Claims submitted under the new group before that enrollment is complete will be denied.
- Credentialing lapse due to missed recredentialing. Payers require periodic recredentialing, typically every two to three years. If a provider misses a recredentialing deadline, their active status with that payer can lapse, resulting in denials on all subsequent claims until the issue is resolved. This is one of the most preventable credentialing problems and one of the most disruptive when it is caught late.
- Effective date mismatch. Many payers will not pay for services rendered before the provider’s enrollment effective date, even if the enrollment is now active. This is a common source of lost revenue for practices that allow new providers to start seeing patients before enrollment is confirmed.
- Registration errors that mimic credentialing problems. Sometimes a claim fails because the patient’s insurance information was entered incorrectly at registration, the wrong plan was selected, or the patient’s coverage was inactive on the date of service. These issues show up in billing as credentialing-related denials but are actually front-end registration problems that need to be corrected at the source.
A Practical Claim Review Framework
When a claim comes back with a credentialing-related denial, a structured review process keeps the investigation from becoming chaotic.
Here is a step-by-step approach that works across practice sizes and specialties:
- Step 1: Pull the full denial reason. Do not stop at the denial code. Read the full explanation of benefits or remittance advice to get the specific language the payer used. “Provider not on file,” “rendering provider not eligible,” and “group not contracted” all point to different problems requiring different solutions.
- Step 2: Confirm the rendering provider’s current enrollment status. Contact the payer directly or check the payer’s provider portal to confirm whether the rendering provider is actively enrolled, when their enrollment became effective, and whether there are any flags or pending items on their account.
- Step 3: Verify the NPI and tax ID on the claim. Pull the original claim and check that the correct NPIs appear in the correct fields. Confirm that the tax ID matches what the payer has on file for the group.
- Step 4: Check the date of service against the enrollment effective date. If the service was rendered before the enrollment effective date, determine whether the payer allows retroactive billing. If it does not, this revenue may not be recoverable, which is important to document for future planning.
- Step 5: Determine whether the issue is credentialing, enrollment, or billing. Based on what you find in steps one through four, classify the problem accurately. This determines who needs to fix it and how.
- Step 6: Assign ownership and set a resolution timeline. Credentialing and enrollment issues go to the credentialing team. Billing and coding errors go to the billing team. Registration problems go to the front office. Every denied claim in this category should have a named owner and a deadline.
Collaboration and Escalation Best Practices
The biggest reason credentialing-related claim issues drag on is a lack of communication between departments. Billing teams often do not know what stage a provider’s enrollment is in. Credentialing teams often do not know which payers are generating the most denials. Neither team has the full picture, and claims fall through the gaps as a result.
A few practices that help close that gap:
- Hold a regular cross-department meeting. A short weekly or biweekly meeting between billing and credentialing to review open denials, discuss upcoming provider starts, and flag any enrollment deadlines prevents a lot of problems from becoming expensive surprises.
- Build a provider onboarding checklist. Before any new provider sees their first patient, there should be a documented checklist confirming enrollment status with every relevant payer. Providers should not be scheduled for insured patients until that checklist is complete.
- Track enrollment effective dates proactively. Maintain a running log of every provider’s enrollment status with every active payer, including the effective date and the next recredentialing date. Review this log monthly.
- Create a denial escalation path. When a credentialing-related denial cannot be resolved at the billing level, there should be a clear path for escalating it to the credentialing team, with defined response times and documentation requirements.
- Document everything. Every call with a payer, every portal check, every application submission should be documented with dates and reference numbers. This documentation is essential when appealing denials or resolving disputes about enrollment timelines.
Keeping Your Practice Compliant and Fully Credentialed
Staying credentialed and enrolled is not a one-time event. It is an ongoing process that requires consistent attention.
Here are the most important things practices can do to stay current:
- Monitor license and certification expiration dates for every provider and build renewals into your calendar well in advance.
- Track recredentialing cycles with each payer and start the process at least 90 days before the deadline.
- Update CAQH ProView profiles regularly. Many payers pull from CAQH during credentialing, and outdated information there can slow down or derail applications.
- Notify payers promptly when provider information changes, including address, group affiliation, or specialty.
- Keep copies of all executed payer contracts and confirm that the rates and terms on file match what is actually being reimbursed.
Compliance is not only about avoiding denials. It is about protecting your ability to bill at all. A provider whose credentials lapse with a major payer can create a billing gap that takes months to resolve, and the revenue lost during that period is often unrecoverable.
Key Takeaways
 Credentialing and revenue cycle management work best when they work together. The practices that handle credentialing-related claim issues most efficiently are the ones that treat these two functions as connected, not separate, and that build the communication structures to support that connection.
Credentialing and revenue cycle management work best when they work together. The practices that handle credentialing-related claim issues most efficiently are the ones that treat these two functions as connected, not separate, and that build the communication structures to support that connection.
A true credentialing problem requires a credentialing solution. A billing error requires a billing solution. A registration problem requires a registration solution. Getting that distinction right, and having a clear framework for making it, saves time, protects revenue, and reduces the frustration that comes with chasing denials that nobody fully owns.
Frequently Asked Questions
- What is the difference between credentialing and enrollment? Credentialing verifies a provider’s qualifications, including licensure, training, and professional history. Enrollment is the process of registering that provider with a specific insurance company so they can bill and receive payment. A provider must complete both before claims can be successfully processed with any given payer.
- How long does payer enrollment typically take? Timelines vary by payer, but most commercial enrollments take between 60 and 120 days. Some payers, particularly Medicaid managed care organizations, can take longer. Starting the enrollment process well before a provider’s anticipated start date is essential to avoiding billing gaps.
- Can a practice bill retroactively once enrollment is approved? Some payers allow retroactive billing back to the provider’s application date or credentialing approval date, but many do not. This should be confirmed directly with each payer before services are rendered, and practices should hold claims rather than submit them with the expectation of retroactive payment unless that policy has been verified.
- What should I do if a payer says a provider is “not on file”? Start by confirming that the enrollment application was submitted and received. Check the payer portal or call provider relations to verify enrollment status. If the application is pending, get an estimated timeline and document the contact. If the application was never received, determine whether it was submitted and lost or never submitted in the first place, and resubmit immediately with proof of the original submission if available.
- How often does a provider need to be recredentialed? Most payers require recredentialing every two to three years. Hospitals typically follow the same cycle. Missing a recredentialing deadline can result in termination from the payer network, which means all subsequent claims will be denied until the provider’s status is reinstated.
- What is CAQH ProView and why does it matter? CAQH ProView is a centralized database that providers use to store and share their credentialing information with participating payers. Keeping a CAQH profile current and attested regularly speeds up the credentialing and recredentialing process significantly, because payers pull directly from it rather than requiring providers to submit the same information repeatedly.
Summary: Revenue Cycles are Affected by Credentialing and Enrollment
![]() Credentialing and enrollment are not back-office formalities. They are the infrastructure that makes billing possible, and when they break down, the revenue cycle breaks down with them. The practices that protect their revenue most effectively are the ones that treat credentialing as an active, ongoing function rather than a one-time box to check, and that build real communication between credentialing and billing teams so problems get caught before they become denials.
Credentialing and enrollment are not back-office formalities. They are the infrastructure that makes billing possible, and when they break down, the revenue cycle breaks down with them. The practices that protect their revenue most effectively are the ones that treat credentialing as an active, ongoing function rather than a one-time box to check, and that build real communication between credentialing and billing teams so problems get caught before they become denials.
Medwave provides medical billing, credentialing, and payer contracting services to healthcare practices of all sizes and specialties across the United States. Whether you need help managing provider enrollment, resolving credentialing-related claim denials, or renegotiating payer contracts to improve your reimbursement rates, our team brings the expertise and the follow-through to get it done. Reach out to Medwave today to find out how we can support your revenue cycle from the ground up.