
Claim denials are one of those problems that healthcare organizations tend to accept as part of doing business. They happen, someone works them, some get paid, some get written off, and the cycle repeats. What rarely gets examined is the real cost of that cycle, not just the individual denied claims, but the cumulative revenue leak that builds up month after month when denials are treated as inevitable rather than preventable.
The organizations that reverse that trend share one thing in common. They stopped being reactive. Instead of waiting for denials to arrive and then scrambling to appeal them, they built systems designed to stop denials before they happen. That shift, from reactive damage control to proactive revenue integrity, is where the real financial gains are.
Why Revenue Integrity is Crucial to Measure
 Revenue integrity is a term that gets used in a lot of different ways, so it is worth being specific about what it actually means in practice. At its core, revenue integrity is about making sure that every service a provider delivers is accurately documented, correctly coded, properly billed, and fully reimbursed. It sits at the intersection of clinical documentation, coding accuracy, billing operations, and compliance.
Revenue integrity is a term that gets used in a lot of different ways, so it is worth being specific about what it actually means in practice. At its core, revenue integrity is about making sure that every service a provider delivers is accurately documented, correctly coded, properly billed, and fully reimbursed. It sits at the intersection of clinical documentation, coding accuracy, billing operations, and compliance.
The revenue integrity function bridges the gap between what happens clinically and what gets submitted to a payer. When clinical documentation does not support the codes being billed, denials follow. When coding does not reflect the actual services provided, revenue is either left on the table or at risk of being flagged for overpayment. Revenue integrity work closes those gaps before a claim ever leaves the building.
A well-functioning, critical revenue integrity program does several things simultaneously. It monitors denial patterns and traces them back to their origin. It works with clinical teams to improve documentation practices at the point of care. It audits coding for accuracy and compliance. And it tracks payer behavior over time, identifying which payers are denying which claim types and why, so that internal processes can be adjusted accordingly.
Why Denials Deserve More Attention Than They Usually Get
Most healthcare organizations track their denial rate. Fewer track what those denials actually cost in total, including the staff time spent on appeals, the claims that never get recovered, the cash flow delays while disputes sit in queue, and the write-offs that accumulate quietly in the background.
Industry estimates consistently put denial rates between 5 and 10 percent of submitted claims for most organizations, with some specialties running higher. On paper, that might not sound alarming. In practice, for a mid-sized practice or health system, that percentage represents a significant chunk of revenue that was earned, billed, and then not collected. And because the cost of reworking a denied claim is substantially higher than submitting a clean claim in the first place, the financial hit compounds.
The other issue is that denials are not random. They follow patterns. The same coding errors, the same documentation gaps, the same eligibility oversights tend to generate denials over and over again. That means every unaddressed root cause is not just one problem but an ongoing one that will keep producing denied claims until someone fixes it at the source.
The Root Cause Problem
 One of the most important shifts in denial management thinking over the past decade is the move from managing individual denials to identifying and eliminating root causes. The difference matters enormously in terms of results. Many billing platforms have installed a denials predictor or rules engine (artificial intelligence) to identify and weed out these types of causes.
One of the most important shifts in denial management thinking over the past decade is the move from managing individual denials to identifying and eliminating root causes. The difference matters enormously in terms of results. Many billing platforms have installed a denials predictor or rules engine (artificial intelligence) to identify and weed out these types of causes.
Managing individual denials means appealing each one as it arrives, recovering what you can, and writing off the rest. It is time-consuming, it keeps billing staff perpetually behind, and it does nothing to prevent the same denial from happening again next month.
Identifying root causes means asking a different question: not just “why was this claim denied” but “why do we keep getting denials like this one?” The answer might be a specific documentation deficiency in a particular service line, a credentialing gap that leaves certain providers out of network with a specific payer, an eligibility verification process that misses certain plan types, or a coding pattern that does not align with a payer’s current policies.
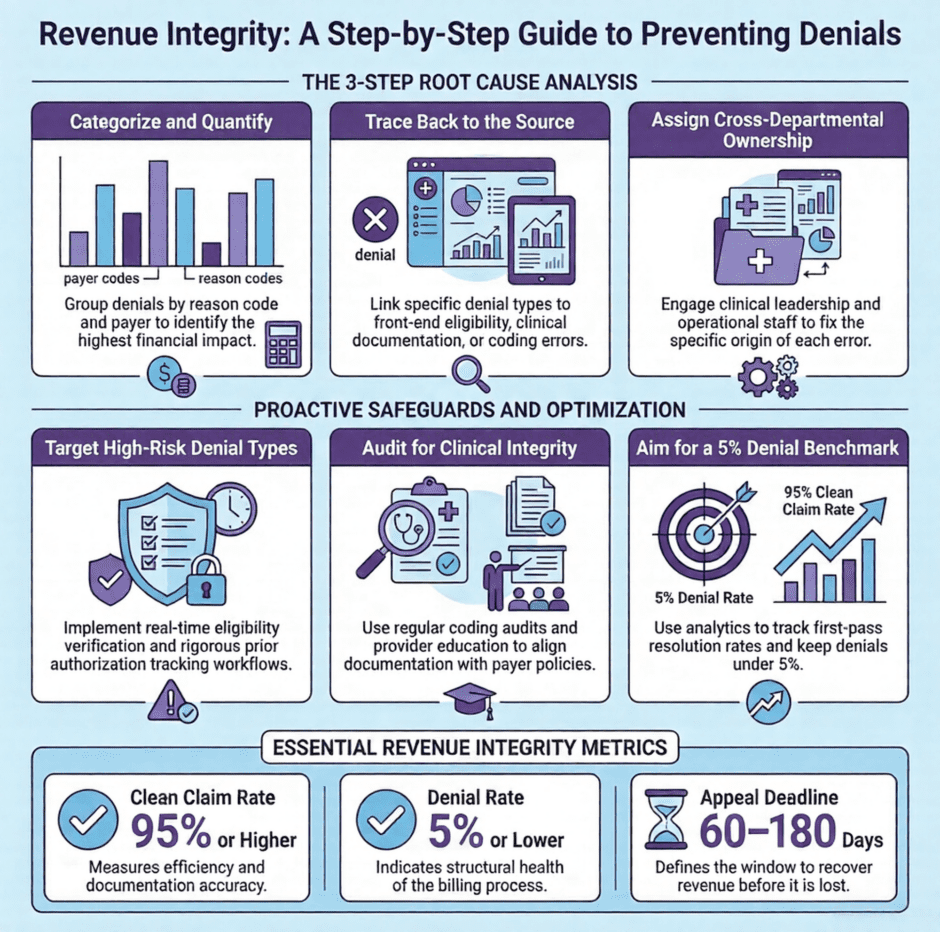
Here is a practical framework for approaching root cause analysis in denial management:
- Categorize denials by type. Group denied claims by denial reason code and payer. Volume by category reveals where the biggest problems are concentrated.
- Trace each category back to its source. For coding denials, the trail leads to documentation and coder behavior. For eligibility denials, it leads to front-end verification processes. For authorization denials, it leads to workflows around prior auth management.
- Quantify the financial impact by category. Not all denial types are equal in terms of recovery potential or prevention difficulty. Prioritizing by dollar value and recurrence rate focuses resources where they matter most.
- Assign ownership for each root cause. Denials that originate in clinical documentation require clinical engagement. Denials that originate in front-end processes require operational fixes. Revenue integrity work that does not cross departmental lines rarely moves the needle.
Building a Denial Management Program That Actually Works
 A lot of organizations have something they call a denial management program. Fewer have one that functions as a genuine revenue recovery and prevention engine. The difference is usually in the structure, the data, and the cross-departmental engagement.
A lot of organizations have something they call a denial management program. Fewer have one that functions as a genuine revenue recovery and prevention engine. The difference is usually in the structure, the data, and the cross-departmental engagement.
Structure matters because denials touch every part of the revenue cycle. A denial management program that lives only in the billing department will always be fighting with one hand tied behind its back. Effective programs have governance that includes clinical leadership, coding and HIM staff, compliance, finance, and operations. Each group has a role to play, and sustainable improvement requires all of them to be engaged.
Data matters because you cannot manage what you cannot measure. Organizations that are serious about denial management invest in analytics tools that track denial rates by payer, by service line, by provider, by denial reason code, and over time. Trends become visible. Outliers get flagged. The impact of process changes can be measured. Without that data infrastructure, denial management is mostly guesswork dressed up as action.
Communication matters because the people who create documentation and order services often do not see the downstream billing consequences of what they do. Bringing clinical teams into the conversation, sharing denial data with physicians and clinical staff in formats that are accessible and relevant to them, and building feedback loops between the billing operation and the clinical floor are all practices that make a meaningful difference over time.
Preventing High-Risk Denial Types
Some denial types are more preventable than others, and focusing prevention efforts on the highest-risk categories produces the best return.
The usual suspects include:
- Authorization denials
Services rendered without the required prior authorization or with an expired one. Prevention requires a tight workflow around authorization management, including tracking authorization validity periods, aligning authorized services with what is actually being provided, and proactive follow-up before authorizations expire. - Eligibility and coverage denials
Claims submitted for patients whose coverage was inactive, terminated, or different from what was on file. Real-time eligibility verification at the front end of every encounter is the primary defense here, combined with a process for updating insurance information when patients report changes. - Coding and documentation denials
Claims denied because the documentation does not support the level of service billed, or because codes were applied incorrectly. Regular coding audits, provider education, and clinical documentation improvement programs address this category at the source.
Each of these denial types has a clear prevention pathway. The investment in prevention almost always costs less than the repeated cost of reworking and appealing the denials they generate.
Using Data and Analytics to Drive Continuous Improvement
 The organizations that sustain low denial rates over time are the ones that treat data as a management tool, not just a reporting function. Analytics in denial management is not about generating dashboards for their own sake. It is about identifying patterns, measuring the impact of interventions, and making decisions based on evidence rather than intuition.
The organizations that sustain low denial rates over time are the ones that treat data as a management tool, not just a reporting function. Analytics in denial management is not about generating dashboards for their own sake. It is about identifying patterns, measuring the impact of interventions, and making decisions based on evidence rather than intuition.
Key metrics worth tracking consistently include overall denial rate by payer and service line, first-pass resolution rate, denial overturn rate on appeal, average days to resolution for denied claims, write-off rate by denial category, and cost to collect on denied versus clean claims. Watching these numbers over time, and correlating them with specific process changes, builds an evidence base for what is working and what needs further attention.
Predictive analytics takes this a step further, using historical denial data to flag claims at high risk of denial before they are submitted. Some practice management and revenue cycle platforms now offer this capability. When a claim gets flagged as high-risk before it goes out the door, the billing team has an opportunity to correct it proactively rather than deal with the denial after the fact.
FAQs: Revenue Integrity and Denial Management
- What is the difference between denial management and revenue integrity?
Denial management is the process of responding to denied claims, appealing them, and recovering revenue after the fact. Revenue integrity is broader. It encompasses the proactive work done before claims are submitted to ensure that documentation, coding, and billing are accurate and compliant. Revenue integrity reduces the volume of denials that need to be managed in the first place. - What is a realistic denial rate benchmark for a well-run practice?
Industry benchmarks generally target a clean claim rate of 95 percent or higher, which translates to a denial rate at or below 5 percent. Many organizations run higher than that, particularly in specialties with frequent prior authorization requirements or complex coding. A denial rate consistently above 10 percent is a signal that something structural needs attention. - How do you prioritize which denials to work first?
The most common approach is to prioritize by dollar value and by appeal deadline. High-dollar denials with approaching timely appeal windows get worked first. Beyond that, grouping denials by category and working them in batches is more efficient than addressing each one individually, and it surfaces the root causes faster. - What role does clinical documentation play in reducing denials?
A significant one. A large share of coding and medical necessity denials trace back to documentation that does not adequately support the services billed. Physician and clinical staff education about documentation requirements, combined with real-time feedback from coding and revenue integrity teams, addresses the problem at its source rather than downstream in the billing operation. - Can a small practice build an effective denial management program?
Yes, though the scale looks different. A small practice may not have a dedicated revenue integrity team, but it can still implement systematic denial tracking, regular coding audits, consistent eligibility verification, and authorization management workflows. Outsourcing billing to a company with strong denial management capabilities is also a viable option that gives smaller practices access to infrastructure they could not build cost-effectively on their own. - How often should denial trends be reviewed?
Monthly at a minimum. High-volume practices or those with elevated denial rates benefit from weekly reviews of denial categories and appeal statuses. The goal is to catch patterns early enough to make process corrections before a denial type becomes deeply entrenched.
People Also Ask
- What causes most claim denials in medical billing?
The most common causes include insurance eligibility issues, missing or expired prior authorizations, coding errors or mismatches between diagnosis and procedure codes, documentation that does not support the level of service billed, and timely filing violations. Most of these are preventable with strong front-end processes and regular internal audits. - How long does a provider have to appeal a denied claim?
Appeal deadlines vary by payer and by contract. Most commercial payers allow between 60 and 180 days from the date of the denial to file an appeal. Medicare has its own appeal timeline, which starts with a redetermination request that must be filed within 120 days of receiving the initial determination. Missing appeal deadlines typically forfeits the right to recover the claim. - What is a revenue integrity department in a hospital or health system?
A revenue integrity department is a team focused on ensuring that clinical services are accurately documented, coded, and billed to maximize reimbursement while maintaining compliance. It typically sits at the intersection of coding, clinical documentation improvement, compliance, and the billing operation, and it works proactively to prevent revenue leakage rather than just recovering it after denials occur. - Is it worth hiring outside help for denial management?
For many practices and health systems, yes. Denial management requires consistent attention, strong analytics capabilities, and deep knowledge of payer behavior across multiple payers and plan types. Outsourcing to a billing company with dedicated denial management expertise often produces better recovery rates and lower administrative costs than trying to build that capability entirely in-house.
Summary: Turning Denials Into a Managed, Measurable Process
![]() Claim denials will never go away entirely. Payer policies shift, coding guidelines change, and some claims will always require follow-up. But the difference between an organization that writes off 8 to 10 percent of its billed charges and one that consistently holds its denial rate below 5 percent is almost never luck. It is process, data, and the willingness to treat denials as a solvable operational problem rather than an unavoidable cost of doing business.
Claim denials will never go away entirely. Payer policies shift, coding guidelines change, and some claims will always require follow-up. But the difference between an organization that writes off 8 to 10 percent of its billed charges and one that consistently holds its denial rate below 5 percent is almost never luck. It is process, data, and the willingness to treat denials as a solvable operational problem rather than an unavoidable cost of doing business.
The providers and revenue cycle teams that see the strongest results are the ones who invest in prevention, trace problems to their root causes, engage clinical teams in the solution, and use data to measure what is actually working.
At Medwave, we support healthcare providers across the country with medical billing, credentialing, and payer contracting. Our billing work includes active denial management and the kind of systematic follow-up that keeps revenue moving rather than stalling in a queue. If your denial rate is higher than it should be, or if you are spending more time fighting payers than caring for patients, we would be glad to take a closer look at what is driving it. Reach out to our team today.