
Modifier 25 appears on millions of medical claims every year, making it one of the most frequently used modifiers in medical billing. It’s also one of the most frequently audited. Insurance companies scrutinize Modifier 25 claims closely because historically, this modifier has been both misunderstood and misused.
When you use Modifier 25 correctly, you get paid for legitimate evaluation and management services that you performed on the same day as a procedure. When you use it incorrectly, you face claim denials, payment delays, and potential audit problems. The difference often comes down to documentation and knowing exactly when the modifier applies.
This guide walks through everything you need to know about Modifier 25. You’ll learn what “separately identifiable” really means, how to document it properly, which common mistakes to avoid, and how to protect your practice from audit risks while capturing the revenue you’ve earned.
What Modifier 25 Really Means
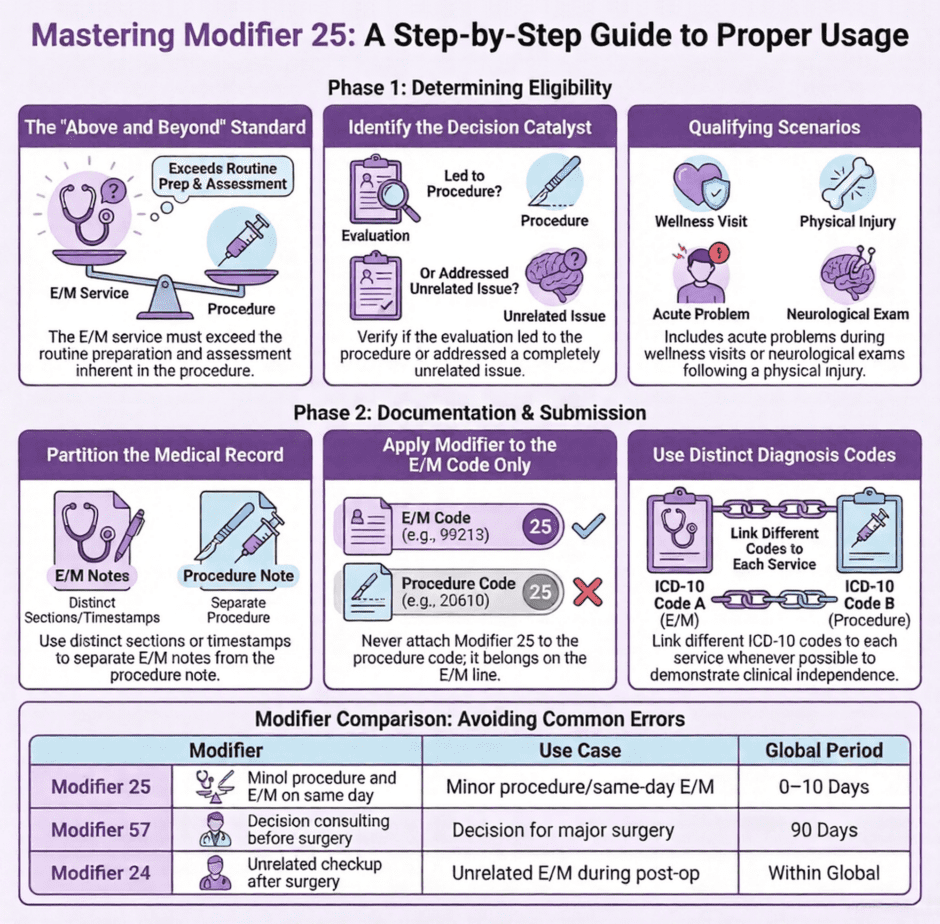
 Modifier 25 identifies a “Significant, Separately Identifiable Evaluation and Management Service by the Same Physician or Other Qualified Healthcare Professional on the Same Day of the Procedure or Other Service.” That’s the official CMS definition, and every word matters.
Modifier 25 identifies a “Significant, Separately Identifiable Evaluation and Management Service by the Same Physician or Other Qualified Healthcare Professional on the Same Day of the Procedure or Other Service.” That’s the official CMS definition, and every word matters.
The key phrase is “separately identifiable.” You’re telling the insurance company that you performed an E/M service that was distinct from the normal work involved in preparing for and performing a procedure. This isn’t about doing two unrelated things. It’s about doing evaluation and management work that goes above and beyond what’s typically included in the procedure itself.
Every procedure code includes some amount of E/M work. When you inject a joint, you need to assess the injection site and get basic consent. When you remove a lesion, you need to identify the correct location and prepare the area. This routine preparation doesn’t qualify for separate billing with Modifier 25. The E/M service must be significant enough and separate enough to stand on its own.
Think of it this way. If the patient came in just for the procedure and you did your normal pre-procedure assessment, that’s included in the procedure payment. But if the patient came in with a problem that required a separate evaluation, and during that evaluation you decided a procedure was necessary, or if they came in for a scheduled procedure but also had an unrelated issue you needed to address, that separate evaluation deserves separate payment.
When Modifier 25 Actually Applies
The most common legitimate use of Modifier 25 happens when a patient presents with a problem requiring evaluation, and during that visit you also perform a procedure. For example, a patient comes to your primary care office complaining of worsening knee pain. You take a detailed history about the pain, examine the knee and surrounding structures, review their medication effectiveness, assess their range of motion, and determine that an injection would provide relief. You then perform the joint injection.
In this scenario, you did real E/M work evaluating the knee problem before deciding on and performing the injection. That evaluation is separately identifiable from the injection procedure itself. The documentation should clearly show the history, examination, and medical decision-making that led to your treatment plan, which included the injection.
Another common scenario involves preventive visits with acute problems. A patient comes in for their annual physical. During the well visit, they mention they’ve been having chest pain. You need to evaluate that chest pain separately from the preventive exam. You take additional history about the chest pain characteristics, perform a focused cardiovascular exam beyond the routine physical exam elements, and make medical decisions about testing and treatment. This additional work justifies billing both the preventive visit and a separate problem-focused E/M with Modifier 25.
Unrelated problems addressed on the same day as a procedure also qualify. A dermatologist might see a patient for a scheduled skin cancer screening and biopsy of a suspicious lesion. During the visit, the patient asks about worsening eczema on their hands. The physician evaluates the eczema, prescribes treatment, and provides management instructions. That’s a separate E/M service from the skin screening and biopsy.
The “Separately Identifiable” Standard
 This is where most confusion and audit problems occur. Separately identifiable doesn’t just mean you documented two different things. It means the E/M service you provided was distinct from the evaluation inherent in deciding to perform the procedure and preparing for it.
This is where most confusion and audit problems occur. Separately identifiable doesn’t just mean you documented two different things. It means the E/M service you provided was distinct from the evaluation inherent in deciding to perform the procedure and preparing for it.
Documentation must show you performed history, examination, and medical decision-making that goes beyond what any reasonable physician would do as part of the procedure. If you’re billing a laceration repair, you obviously need to look at the laceration, assess its depth and complexity, and decide on the repair method. That’s included in the laceration repair code. But if the patient fell and hit their head, and you also perform a full neurological assessment to rule out concussion, that’s separately identifiable work.
The concept of “above and beyond” helps clarify this. Ask yourself, did I do more evaluation and management than what’s typically required for this procedure? Did I address issues unrelated to the procedure? Did I perform a distinct evaluation of a problem that led to the decision to do the procedure?
Here’s what doesn’t meet the separately identifiable standard. A patient schedules an appointment for a joint injection. When they arrive, you confirm the correct joint, verify they still want the injection, and perform your standard pre-injection assessment. Then you do the injection. That pre-injection work is built into the injection code. There’s no separate E/M service to bill, even if it took you 10 minutes.
Documentation That Supports Modifier 25
Your medical record must clearly show the separately identifiable E/M service. The best approach is to document the E/M portion separately from the procedure. Use distinct sections in your note or different time stamps. Make it obvious to anyone reviewing the chart that you performed substantial evaluation and management work independent of the procedure.
For the E/M service, document the key elements:
- Chief complaint or reason for the E/M portion of visit
- History of present illness for the problem being evaluated
- Review of systems relevant to the problem
- Examination of body areas and organ systems
- Medical decision-making including assessment and plan
- Time spent if you’re billing based on time
This documentation should stand on its own. Someone reading just the E/M portion should be able to recognize it as a complete evaluation. It shouldn’t reference the procedure or rely on procedure documentation to make sense.
Then separately document the procedure. Include the indication, technique, findings, and patient tolerance. This should read like a procedure note, not an extension of your E/M documentation.
Many practices struggle because their documentation mixes everything together. The note flows from history to exam to “I decided to inject the knee today” with procedure details. This makes it look like the E/M work was just preparation for the procedure rather than a separate service. Clear organization prevents this problem.
When NOT to Use Modifier 25
 Understanding when not to use Modifier 25 is just as important as knowing when to use it. The most common inappropriate use happens when providers add Modifier 25 to every E/M billed on the same day as a procedure, regardless of whether a separately identifiable service actually occurred.
Understanding when not to use Modifier 25 is just as important as knowing when to use it. The most common inappropriate use happens when providers add Modifier 25 to every E/M billed on the same day as a procedure, regardless of whether a separately identifiable service actually occurred.
Standard pre-procedure evaluation doesn’t qualify. If a patient schedules a procedure and you perform your typical assessment before doing it, you can’t bill a separate E/M. The pre-procedure history, consent discussion, site verification, and basic examination are all included in the procedure payment.
Similarly, post-procedure checks on the same day are included in the procedure. After you complete a minor surgical procedure, you check the site, provide wound care instructions, and ensure the patient is stable. This is part of the procedure, not a separate E/M service.
Follow-up visits within the global period of a surgery can’t use Modifier 25. These visits are covered by the original surgical payment. The exception is if you’re seeing the patient for a completely unrelated problem during the post-op period, in which case you’d use Modifier 24, not Modifier 25.
Another common error is using Modifier 25 when the same diagnosis is on both the E/M and the procedure, with no documentation showing what made the E/M separately identifiable. While you can use the same diagnosis for both services in certain situations, your documentation must clearly show why the E/M work was distinct from procedure preparation.
Modifier 25 vs. Other E/M Modifiers
Modifier 25 often gets confused with Modifier 57, but they serve different purposes. Modifier 57 identifies the decision for surgery and applies to major procedures with 90-day global periods (or 10-day global periods for Medicare). Use Modifier 57 when you evaluate a patient and decide they need major surgery, and the surgery happens the next day or within the decision period.
Modifier 25 applies to minor procedures with 0-day or 10-day global periods. If you see a patient, decide they need a minor procedure, and perform it the same day, you use Modifier 25, not Modifier 57.
Modifier 24 is for E/M services during a post-operative period that are unrelated to the original surgery. If a patient is recovering from a knee surgery and comes in with a respiratory infection, you’d bill the sick visit with Modifier 24 to show it’s unrelated to the surgical follow-up.
You apply Modifier 25 to the E/M code, never to the procedure code. This is a common billing error. On your claim form, the E/M code (like 99213 or 99214) gets Modifier 25. The procedure code appears on a separate line without the modifier.
Real-World Examples
 A primary care scenario might look like this. Mrs. Johnson has an appointment for her diabetes follow-up. During the visit, you review her blood sugar logs, adjust her medication, discuss diet and exercise, and address diabetic foot care. While examining her, you notice a large skin tag on her neck that’s getting irritated from her necklace. She asks if you can remove it. You assess the skin tag, confirm it’s appropriate for simple removal, and remove it during the same visit.
A primary care scenario might look like this. Mrs. Johnson has an appointment for her diabetes follow-up. During the visit, you review her blood sugar logs, adjust her medication, discuss diet and exercise, and address diabetic foot care. While examining her, you notice a large skin tag on her neck that’s getting irritated from her necklace. She asks if you can remove it. You assess the skin tag, confirm it’s appropriate for simple removal, and remove it during the same visit.
You bill the established patient E/M code with Modifier 25 for the diabetes management, and you bill the skin tag removal separately. Your documentation shows a complete E/M note addressing the diabetes care, then a separate procedure note for the skin tag removal. The E/M work for the diabetes management is clearly distinct from the simple decision to remove an irritated skin tag.
In dermatology, a patient schedules a full body skin check due to a family history of melanoma. You perform a thorough skin examination, identify several benign lesions, and find one suspicious lesion on the back that needs biopsy. You also spend time discussing sun protection strategies and reviewing what changes to watch for. During the visit, the patient mentions persistent facial redness and asks about it. You examine the facial skin, diagnose rosacea, and prescribe treatment.
You bill the skin check E/M with Modifier 25, the biopsy, and you might include discussion of the rosacea in the same E/M or bill it separately depending on the extent of evaluation. The key is that your skin examination and assessment went beyond simply identifying which lesion to biopsy.
An incorrect example shows the difference. A patient calls saying they need a cortisone injection for their inflamed knee. They schedule an injection appointment. When they arrive, you verify which knee hurts, examine the knee to confirm the injection site, obtain consent, and perform the injection. This doesn’t justify an E/M with Modifier 25. You only did the evaluation necessary for the procedure. Your documentation would struggle to show separately identifiable E/M work because there wasn’t any.
Audit Risks and Compliance
Modifier 25 attracts significant audit attention because it directly increases reimbursement. When you bill an E/M with a procedure instead of just the procedure, you receive substantially more payment. Auditors look for patterns that suggest inappropriate modifier use.
Red flags include using Modifier 25 on a very high percentage of your procedures, consistently billing high-level E/M codes when you also perform procedures, and frequently using the same diagnosis for both the E/M and procedure without clear documentation of distinct services.
To prepare for potential audits, conduct internal reviews of your Modifier 25 usage. Pull a sample of claims where you used the modifier and review the documentation. Can you clearly identify the separately identifiable E/M service? Is it documented in a way that would satisfy an auditor? If not, you need to improve either your documentation or your billing practices.
Provider education is critical. Physicians often don’t realize that what they consider a thorough pre-procedure assessment is actually just standard preparation included in the procedure payment. They need to learn what constitutes a separately identifiable service and how to document it properly. Regular feedback on documentation quality helps providers improve.
Create written policies for your practice that define when Modifier 25 is appropriate. Include specialty-specific scenarios that commonly occur in your setting. Make sure everyone involved in coding and billing knows these guidelines and follows them consistently.
Preventive Visits with Problem Management
 One of the most common Modifier 25 scenarios involves preventive services. Medicare and most commercial payers allow you to bill both a preventive visit and a problem-focused E/M on the same day when medically appropriate. The preventive visit addresses health maintenance, screening, and counseling. The problem E/M addresses acute or chronic conditions requiring evaluation and management.
One of the most common Modifier 25 scenarios involves preventive services. Medicare and most commercial payers allow you to bill both a preventive visit and a problem-focused E/M on the same day when medically appropriate. The preventive visit addresses health maintenance, screening, and counseling. The problem E/M addresses acute or chronic conditions requiring evaluation and management.
Documentation for these visits should clearly separate the two services. The preventive portion documents age and gender-appropriate screening, immunizations, counseling, and review of health maintenance items. The problem-focused portion documents the chief complaint, history, examination, and medical decision-making for the specific condition.
Most payers require different diagnoses on the preventive visit and the problem E/M. The preventive visit uses a wellness diagnosis code (Z00.00 or similar). The problem E/M uses the diagnosis for the condition being managed. This diagnosis separation helps demonstrate that these were truly distinct services.
Patient communication matters here. Some insurance plans don’t cover problem E/M visits on the same day as preventive care, or they apply cost-sharing to the problem visit. Your front office should verify coverage and help patients decide whether to address acute problems during their wellness visit or schedule a separate appointment.
Getting Expert Billing Help via Medwave
![]() Modifier 25 represents just one aspect of medical billing compliance. Between modifier rules, coding updates, payer policy variations, and documentation requirements, keeping up with billing best practices is a full-time job. Many practices find that professional billing support delivers better results with less stress than trying to manage everything in-house.
Modifier 25 represents just one aspect of medical billing compliance. Between modifier rules, coding updates, payer policy variations, and documentation requirements, keeping up with billing best practices is a full-time job. Many practices find that professional billing support delivers better results with less stress than trying to manage everything in-house.
Medwave specializes in medical billing alongside credentialing and payer contracting services. We ensure all three functions work seamlessly. When credentialing is complete, we have your providers set up correctly in billing systems. When you negotiate payer contracts, we make sure our billing practices align with contract terms. This integration prevents the disconnects that often occur when different vendors handle these functions separately.
Our billing experts stay current with modifier requirements, payer policies, and coding changes so you don’t have to. We review claims before submission to catch potential issues, ensure proper modifier use, and maximize your legitimate reimbursement while maintaining compliance. Our clients report fewer denied claims, faster payment cycles, and significantly reduced audit risk when we manage their billing. We conduct regular internal audits of modifier usage, provide documentation feedback to providers, and help practices develop policies that protect revenue while ensuring compliance.
If you’re concerned about your Modifier 25 usage, facing high denial rates, or simply want to ensure you’re capturing all the revenue you’ve earned, contact Medwave for a free billing compliance assessment. We’ll review your modifier usage patterns, identify opportunities for improvement, and show you exactly how professional billing support can benefit your practice.
Modifier 25 doesn’t have to be a source of confusion and denied claims. With proper documentation, clear policies, and attention to the “separately identifiable” standard, you can use this modifier confidently to receive appropriate payment for the services you provide. The key is knowing the rules, following them consistently, and creating documentation that clearly demonstrates when separate E/M services deserve separate payment.