
General surgery is one of the broadest surgical specialties in medicine, and the billing that comes with it reflects that. On any given day, a general surgeon might perform a laparoscopic cholecystectomy, remove a hernia, biopsy a suspicious mass, manage a wound, and see patients in clinic for post-operative follow-up. That range of services is what makes general surgery so essential to healthcare. It is also what makes general surgery billing one of the more demanding areas in surgical revenue cycle management.
The CPT codes used in general surgery span abdominal procedures, hernia repairs, breast surgery, endoscopy, wound management, soft tissue tumor removals, and a full range of evaluation and management visits. Each category has its own coding logic, documentation requirements, and payer rules. Throw in global surgery periods, assistant surgeon billing, surgical modifier requirements, and prior authorization for elective procedures, and you have a billing environment where small errors can add up to significant lost revenue fast.
We cover how general surgery billing works across the major procedure categories, what credentialing looks like for general surgeons, where common compliance risks tend to show up, and what your practice can do to get claims right the first time.
TL;DR: General surgery billing pulls from dozens of CPT code categories with strict documentation and global period rules. Laparoscopic vs. open approach, primary vs. incidental procedures, and assistant surgeon billing all affect how claims are coded and paid. Credentialing for general surgeons runs through the American Board of Surgery and requires primary source verification of training, licensure, privileges, and malpractice history. Read on for the full breakdown.
How Much Ground Does General Surgery Billing Cover?
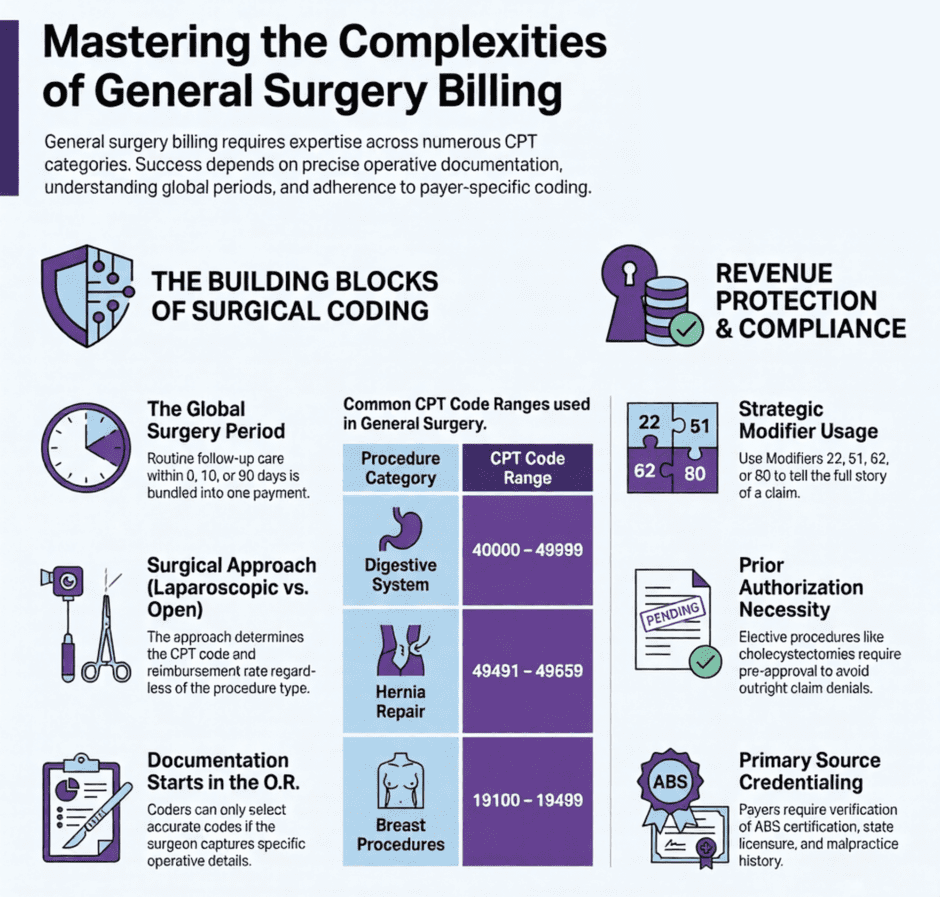
 Most outpatient specialties work from a fairly focused set of CPT codes. General surgery does not work that way. A busy general surgery practice will regularly bill from the digestive system surgery codes in the 40000s through 49999 range, hernia repair codes from 49491 to 49659, breast procedure codes from 19100 to 19499, skin and soft tissue codes from 10000 to 19999, laparoscopy codes scattered throughout the surgical sections, and evaluation and management codes from 99202 to 99215 for clinic visits.
Most outpatient specialties work from a fairly focused set of CPT codes. General surgery does not work that way. A busy general surgery practice will regularly bill from the digestive system surgery codes in the 40000s through 49999 range, hernia repair codes from 49491 to 49659, breast procedure codes from 19100 to 19499, skin and soft tissue codes from 10000 to 19999, laparoscopy codes scattered throughout the surgical sections, and evaluation and management codes from 99202 to 99215 for clinic visits.
Each of those code ranges comes with its own rules. Laparoscopic and open approaches to the same procedure carry different CPT codes and different reimbursement rates. Hernia repair codes are selected based on the type of hernia, whether it is initial or recurrent, and the patient’s age. Getting any of those variables wrong means submitting a code that does not match the documentation, which leads to denials, underpayments, or in more serious situations, compliance risk.
The real challenge for general surgery practices is that most of these distinctions live in the operative report itself. A coder can only select the right code if the surgeon’s documentation captures the right details. That means the billing process in general surgery starts in the operating room, not the billing department.
Global Surgery Periods: The Rule That Shapes Everything
If there is one concept that affects general surgery billing more than any other, it is the global surgery period. Medicare and most commercial payers assign a global period to surgical procedures, either 0 days, 10 days, or 90 days, during which routine follow-up care is considered part of the original procedure payment and cannot be billed separately.
For most major general surgery procedures, that global period is 90 days. That means the pre-operative visit the day before surgery, the surgery itself, and all routine post-operative visits within 90 days are bundled into one payment. Billing a follow-up office visit during the global period for routine wound checks or standard post-op care will result in a denial.
There are situations where services during the global period are separately billable. Treating a complication that requires a return to the operating room, managing a new and unrelated condition, or providing care that goes beyond routine post-operative management can all support a separate claim with the right modifier attached. The key is making sure the documentation clearly supports why that service was separate from the original surgical episode.
Practices that do not track global periods carefully end up with one of two problems. Either they bill for services that are bundled and get denied, or they fail to bill for legitimately separate services because no one recognized that the global period exception applied.
Laparoscopic vs. Open: Why the Approach Determines the Code
 General surgery is one of the specialties where the surgical approach matters a great deal for billing purposes. Laparoscopic and open versions of the same procedure are assigned different CPT codes, and they reimburse differently.
General surgery is one of the specialties where the surgical approach matters a great deal for billing purposes. Laparoscopic and open versions of the same procedure are assigned different CPT codes, and they reimburse differently.
Take cholecystectomy as an example. A laparoscopic cholecystectomy is billed under CPT 47562 or 47563, depending on whether the common bile duct was explored. An open cholecystectomy uses different codes entirely. If a surgeon starts laparoscopically and converts to open during the same procedure, the open code is reported, and the conversion should be documented in the operative report.
The same logic applies to hernia repairs, colectomies, appendectomies, and many other general surgery procedures. The operative report needs to describe the approach taken, any conversion that occurred, and the reason for the approach selected. Documentation that does not clearly state whether the procedure was performed laparoscopically or open forces the coder to make assumptions, which creates both coding errors and potential compliance issues.
Hernia Repair Billing
Hernia repair is one of the highest-volume procedures in general surgery, and the coding for it is more involved than many practices realize. The correct CPT code depends on four things. The type of hernia, the anatomical location, whether it is an initial repair or a recurrent one, and whether the hernia was reducible, incarcerated, or strangulated.
Inguinal hernia repairs, for example, use different codes for initial versus recurrent presentations, and the codes also separate by patient age for pediatric cases. Ventral and incisional hernia codes are selected based on whether the hernia is initial or recurrent and the size of the defect. Umbilical hernia codes separate by defect size and patient age.
A few things worth knowing about hernia billing in particular:
- Recurrent hernia codes reimburse at a higher rate than initial hernia codes, reflecting the added difficulty of operating in a previously repaired field. The documentation needs to clearly state that this is a recurrent hernia, not just a larger or more difficult one.
- Mesh use does not change the CPT code for most hernia repairs. Mesh is considered part of the procedure and is not separately billable in most situations. There are a small number of exceptions, but they require specific documentation.
- Bilateral hernia repairs performed in the same session use Modifier 50 and are reimbursed at a higher combined rate than a single repair. The operative report must clearly document that both sides were repaired during the same encounter.
- Strangulated or incarcerated hernias use different codes than reducible hernias of the same type. The clinical status of the hernia at the time of repair needs to be clearly documented to support the correct code selection.
Abdominal Surgery: Appendectomy, Colectomy, etc.
 The abdominal surgery codes make up a large portion of general surgery billing. Appendectomy, colectomy, small bowel resection, gastrectomy, and related procedures each have their own CPT codes, and many of them separate by approach, extent of resection, and presence of complications.
The abdominal surgery codes make up a large portion of general surgery billing. Appendectomy, colectomy, small bowel resection, gastrectomy, and related procedures each have their own CPT codes, and many of them separate by approach, extent of resection, and presence of complications.
For appendectomy, CPT 44950 covers an open approach, while 44970 is used for laparoscopic appendectomy. If a ruptured or perforated appendix is found and treated, the documentation needs to reflect that clearly, as it affects the diagnosis code submitted with the claim.
Colectomy codes in the 44140 to 44160 range cover partial colectomies, while total and proctocolectomy procedures use higher-numbered codes. Each code in this range specifies the extent of resection and whether an anastomosis was performed or an ostomy created. The operative report needs to describe those details specifically enough that the coder can select the correct code without guessing.
One area where general surgery practices frequently run into problems is incidental procedures. When a surgeon performs a primary procedure and removes or addresses a secondary finding during the same session, the secondary service is sometimes separately billable and sometimes not. Whether it can be billed separately depends on whether the secondary procedure has its own distinct documentation, a separate indication, and is not considered part of the primary procedure’s work under the NCCI bundling rules.
Evaluation and Management Visits in General Surgery
E/M coding is where general surgery practices lose money most quietly. Surgeons see patients in clinic for new consultations, pre-operative evaluations, and post-operative follow-up, and the documentation does not always reflect the level of service actually provided.
Since the 2021 AMA E/M guideline updates, office visit level selection for established patients (99211 to 99215) is based on either medical decision making or total time. For new patients (99202 to 99205), the same two pathways apply. The old three-element structure is no longer how level selection works for outpatient visits.
Medical decision making for a general surgery clinic visit typically involves the number and nature of problems addressed, data reviewed such as imaging and lab results, and the risk level of the treatment plan being made. A new patient presenting with a large abdominal mass requiring imaging review, multidisciplinary coordination, and surgical planning can legitimately support a level 4 or 5 E/M if the documentation reflects that work. Many surgeons undercode these visits out of habit or caution, which results in ongoing, systematic underpayment.
During the global period, routine post-operative visits are not separately billable. But if a patient comes in for a problem that is unrelated to the surgery, or for evaluation of a complication that requires new clinical decision making beyond standard post-op care, that visit can be billed separately with the right modifier and documentation.
Modifier Use in General Surgery Billing
Modifiers are what tell the payer the full story behind a claim. In general surgery, using the right modifier in the right situation is what separates a paid claim from a denied one.
The modifiers that come up most often in general surgery billing:
- Modifier 22 (Increased Procedural Services) is used when a procedure takes significantly more work than the standard description covers. This could be due to severe adhesions, morbid obesity requiring additional operative time, or other documented factors. The operative report must clearly describe the circumstances that made the procedure more difficult, and the claim should include a brief narrative explaining the increased effort.
- Modifier 51 (Multiple Procedures) applies when more than one surgical procedure is performed in the same operative session by the same provider. The primary procedure is listed without the modifier, and secondary procedures are listed with it. Some codes are exempt from Modifier 51 and retain full value regardless of what else was done.
- Modifier 62 (Two Surgeons) is used when two surgeons from different specialties each perform a distinct part of the same procedure. Both surgeons report the same CPT code with Modifier 62, and payment is split between them. The documentation needs to clearly describe what each surgeon performed.
- Modifier 80 or 82 (Assistant Surgeon) applies when a second surgeon assists during a procedure. Modifier 80 is used when a qualified physician assists. Modifier 82 is used when a qualified resident is not available. Not all payers cover assistant surgeons for all procedures, and prior authorization is sometimes required before the assistant’s services will be reimbursed.
Breast Surgery Billing
 Breast procedures are a significant part of general surgery billing and carry their own specific coding rules. The code range from 19100 to 19499 covers breast biopsies, lumpectomies, mastectomies, and related procedures.
Breast procedures are a significant part of general surgery billing and carry their own specific coding rules. The code range from 19100 to 19499 covers breast biopsies, lumpectomies, mastectomies, and related procedures.
Breast biopsy codes separate by technique. Needle core biopsies use different codes than open biopsies, and image-guided biopsies require specific imaging guidance codes reported alongside the biopsy procedure code. The type of imaging used, whether ultrasound, mammographic, or MRI guidance, determines which guidance code applies.
Mastectomy codes separate by extent of the procedure. Simple mastectomy, modified radical mastectomy, and radical mastectomy each have distinct CPT codes. Skin-sparing and nipple-sparing approaches may also affect coding, depending on the payer. When immediate reconstruction is performed during the same operative session as the mastectomy, the reconstruction codes are separately billable alongside the mastectomy code, and the documentation needs to clearly describe both components.
Prior Authorization in General Surgery
Many payers now require prior authorization for elective general surgery procedures, and the list has grown longer in recent years. Hernia repairs, cholecystectomies, bariatric procedures, and many oncologic surgeries frequently require pre-approval before the payer will process the claim.
Prior authorization requirements vary by payer, by specific plan, and sometimes by the facility where the procedure is being performed. Getting authorization for a procedure at one hospital does not automatically mean the same authorization applies at a different facility.
Failing to get required prior authorization before performing an elective procedure is one of the fastest ways to not get paid. The surgery may have been medically necessary and perfectly performed, but without that prior approval, many payers will deny the claim outright. Building authorization checks into your scheduling workflow, before the procedure is booked rather than after, is the most practical way to avoid that problem.
General Surgery Credentialing Requirements
 Credentialing for general surgeons follows the same general structure as other surgical specialties but with details worth knowing. The primary board certification pathway runs through the American Board of Surgery (ABS), which requires completion of an accredited general surgery residency and passage of both the qualifying and certifying examinations. Some general surgeons also hold additional fellowship training in subspecialties such as colorectal surgery, surgical oncology, hepatobiliary surgery, or minimally invasive surgery, which can affect which procedures are covered by specific payers.
Credentialing for general surgeons follows the same general structure as other surgical specialties but with details worth knowing. The primary board certification pathway runs through the American Board of Surgery (ABS), which requires completion of an accredited general surgery residency and passage of both the qualifying and certifying examinations. Some general surgeons also hold additional fellowship training in subspecialties such as colorectal surgery, surgical oncology, hepatobiliary surgery, or minimally invasive surgery, which can affect which procedures are covered by specific payers.
Primary source verification for a general surgeon covers medical school training, residency and any fellowship completion, ABS certification status, current state licensure in every state where the provider practices, DEA registration, malpractice history, and hospital or surgery center privileges. Each of those credentials is verified directly from the issuing source, not just reviewed from copies provided by the physician.
The NPDB query is a required part of every credentialing application, and any adverse reports must be reviewed before credentialing is complete. Practices that underestimate how long credentialing takes often end up with a new surgeon who is credentialed with the hospital but not yet enrolled with payers, which means weeks or months of revenue either delayed or lost entirely.
Surgical Facility Privileging
General surgeons need procedural privileges at every facility where they operate, separate from payer enrollment. Hospitals and ambulatory surgery centers each have their own privileging processes, and the procedures a surgeon can perform may be limited by their documented training and case volume.
When a surgeon wants to perform a procedure they have not previously been privileged for at a facility, most credentialing committees require documentation of training or a proctored case period before granting the privilege. Starting the privileging application at the same time as payer enrollment, rather than waiting for one to finish before starting the other, can cut months off the timeline before a new surgeon is fully operational.
Payer Contracting and Audit Risk in General Surgery
Payer contracting for general surgery groups is worth approaching with procedure-specific data in hand. Surgery groups have real leverage in contracting conversations, especially when they cover a region with limited surgical access, handle significant oncologic or trauma volume, or provide services across multiple facilities.
Audit risk in general surgery tends to concentrate in these areas:
- Global period billing errors. Billing routine post-operative visits during the global period is one of the most common denial triggers in surgical billing. Equally problematic is failing to use the right modifier when a separately billable service is legitimately performed during the global period.
- Laparoscopic vs. open coding mismatches. Billing a laparoscopic code when the operative report describes an open procedure, or vice versa, is a documentation-to-code mismatch that auditors look for specifically in general surgery.
- Modifier 22 without supporting narrative. Claiming increased procedural services without a clear operative report description of why the case required significantly more work is a red flag for both Medicare and commercial payers. The claim should include a narrative that explains the specific circumstances.
- Assistant surgeon billing without payer authorization. Billing for assistant surgeon services on procedures that a payer does not cover for assistant surgeons, or without the required prior authorization, generates consistent denials and sometimes triggers a broader review of the practice’s billing patterns.
Medicare’s Comprehensive Error Rate Testing program regularly reviews surgical claims, and commercial payers use claims analytics to flag outlier billing patterns. Accurate coding backed by thorough operative documentation is the most effective defense.
General Surgery Billing, Credentialing FAQ
- What CPT codes are most commonly used in general surgery billing?
General surgery pulls from a wide range depending on the services provided. Frequently used code families include hernia repair codes from 49491 to 49659, cholecystectomy codes 47562 and 47563, appendectomy codes 44950 and 44970, colectomy codes from 44140 to 44160, breast procedure codes from 19100 to 19499, soft tissue and skin codes from 10000 to 19999, and E/M codes from 99202 to 99215 for clinic visits. The right code within each family depends on the approach used, the extent of the procedure, and what the operative report documents. - How does the global surgery period affect billing?
The global period bundles pre-operative care, the surgery itself, and routine post-operative follow-up into a single payment. For most major general surgery procedures, the global period is 90 days. Services during that period that go beyond routine post-op care, such as treating a complication or addressing an unrelated condition, can be billed separately with the appropriate modifier and documentation. - Can an assistant surgeon bill separately for the same procedure?
Yes, when the documentation supports it and the payer covers assistant surgeon services for that procedure. The primary surgeon and the assistant surgeon each report the same CPT code with their respective modifiers. Not all payers reimburse assistant surgeons for all procedures, and some require prior authorization before the assistant’s services will be covered. - What board certification do general surgeons need for payer credentialing?
Most payers require certification by the American Board of Surgery. Surgeons with additional fellowship training in subspecialties may need that training documented for specific procedure types to be covered. ABS certification must be verified directly from the board as part of the credentialing process, not just confirmed by self-report. - What triggers a prior authorization requirement for elective surgery?
Prior authorization triggers vary by payer and plan. Most commonly, elective procedures with high cost or significant variation in clinical indication, such as hernia repairs, cholecystectomies, and bariatric surgeries, require pre-approval. The best way to manage this is to verify authorization requirements at the time of scheduling, before the procedure is performed. - What documentation does a general surgery operative report need to support accurate billing?
At a minimum, the operative report should clearly state the surgical approach (laparoscopic or open), the specific procedure performed, the anatomical site, any conversion that occurred and why, the extent of resection if applicable, whether the procedure was initial or recurrent, and any complications encountered. For hernia repairs, the type and reducibility of the hernia should be explicitly documented. For procedures billed with Modifier 22, the report should describe in specific terms why the case required significantly more work than usual.
General Surgeons also Ask
- When is a same-day E/M visit separately billable for a surgical patient?
During a global period, a same-day E/M can be billed separately if it is for a condition completely unrelated to the surgery, or if it involves evaluation and decision making that goes well beyond the standard pre-operative assessment for the procedure performed that day. Modifier 25 is required on the E/M code, and the documentation must clearly reflect that the visit was a distinct service. - How are incidental procedures billed in general surgery?
Whether a secondary procedure performed during the same operative session is separately billable depends on whether it has its own documented indication, whether it requires meaningful additional work, and whether NCCI bundling rules exclude it from separate billing. When a secondary procedure is legitimately separate, Modifier 59 or an XS/XE modifier may be needed to override the bundle. The operative report must describe both procedures independently with clear documentation of each. - Does mesh use in hernia repair generate a separate billing code?
For most hernia repairs, mesh is considered part of the procedure and is not separately billable. There are limited exceptions in specific hernia repair codes where the mesh is factored into a higher-valued code, but those situations require specific documentation and apply to a narrow set of circumstances. Billing mesh as a separate supply item on top of the hernia repair code is a common error that generates denials. - What is the difference between Modifier 62 and Modifier 80 for assistant surgeons?
Modifier 62 is used when two surgeons from different specialties each perform a distinct, separately documented portion of the same procedure. Both surgeons report the same CPT code with Modifier 62, and payment is split. Modifier 80 is used when one surgeon serves as an assistant to the primary surgeon throughout the procedure. The assistant surgeon reports the same CPT code with Modifier 80 and receives a percentage of the primary fee. The two modifiers are not interchangeable. - What are the most common reasons general surgery claims get denied?
The most frequent denial causes in general surgery are global period billing without the correct modifier, laparoscopic vs. open approach mismatches between the operative report and the CPT code, missing or insufficient prior authorization for elective procedures, assistant surgeon billing on procedures the payer does not cover for assistants, and Modifier 22 claims without a supporting narrative. Most of these are preventable with good documentation and a solid pre-billing review process.
How Medwave Supports General Surgery Practices
![]() General surgery billing requires attention to detail at every step. Selecting the right code based on approach and operative findings, managing global periods, applying surgical modifiers correctly, and keeping track of prior authorization requirements all take billers who know general surgery specifically, not just medical billing in general.
General surgery billing requires attention to detail at every step. Selecting the right code based on approach and operative findings, managing global periods, applying surgical modifiers correctly, and keeping track of prior authorization requirements all take billers who know general surgery specifically, not just medical billing in general.
At Medwave, we provide medical billing, provider credentialing, and payer contracting services to general surgery practices and surgical groups across the country. Our billing team works directly with general surgery CPT code sets, operative report documentation standards, and the payer-specific policies that affect your revenue cycle. Our credentialing team manages the full physician credentialing process for general surgeons, including ABS certification verification, multi-state licensure tracking, facility privileging coordination, and PECOS enrollment. Our payer contracting work helps surgery practices negotiate rates and contract terms that reflect the value of what they do, particularly for high-volume procedures and specialized surgical services.
If your general surgery practice has not recently reviewed its coding patterns, modifier usage, or credentialing timelines, that review is worth doing now, before a denial trend or payer audit makes it a more urgent conversation.
Contact Medwave today to schedule a general surgery billing and credentialing review.