
G2211 might be one of the most confusing codes CMS has introduced in recent years. This add-on code went into effect on January 1, 2024, designed to recognize the extra work involved when providers serve as the primary source of ongoing care for patients. The intention was good, but the execution has left many practices scratching their heads about when they can and can’t use it.
The problem is straightforward. CMS created G2211 to capture additional payment for the continuity and coordination work that certain providers do, but they provided minimal guidance on exactly when to report it. The code descriptor talks about visits for “ongoing care related to a patient’s single, serious condition or a complex condition” but doesn’t define what makes something serious or when ongoing care actually begins.
This lack of clarity creates real problems for practices. Bill it too often and you risk audits and payment recoupment. Bill it too rarely and you leave money on the table for legitimate services. Getting it right requires careful attention to the rules, strong documentation, and clear policies about appropriate use.
What G2211 Actually Represents
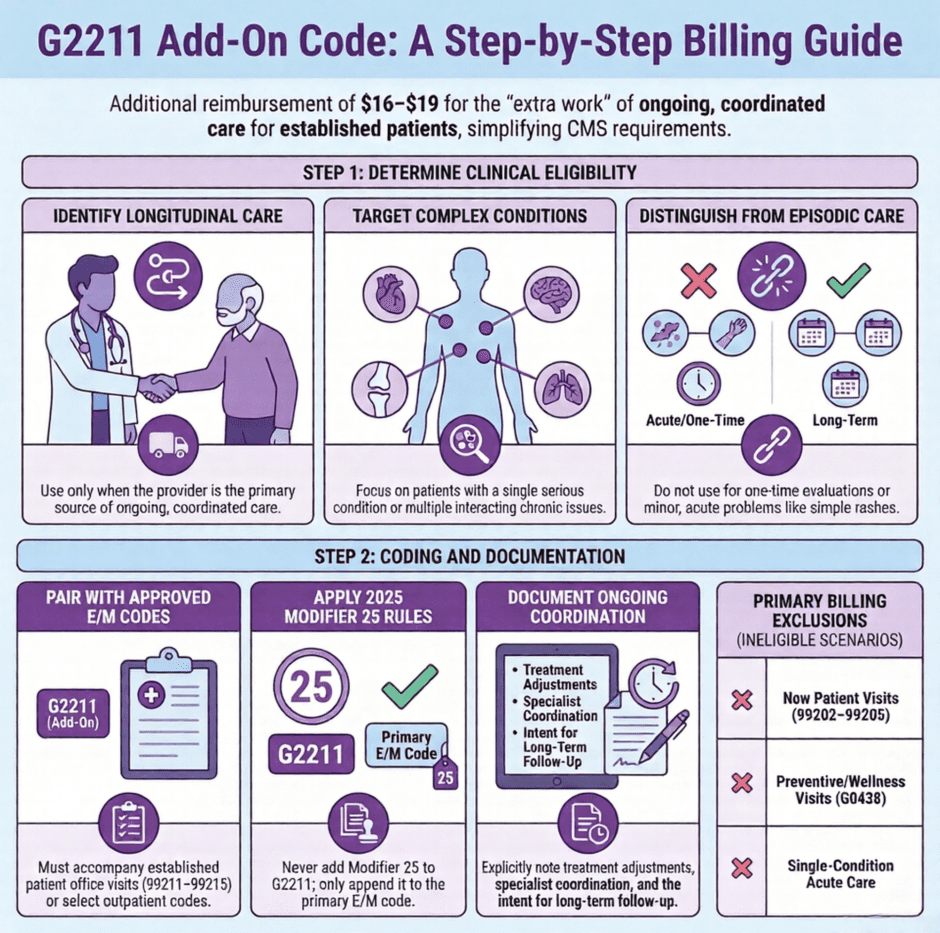
 G2211 is an add-on code, which means you can never bill it alone. It must accompany specific office visit codes for established patients (99211-99215) or certain other outpatient E/M codes. When billed correctly, it adds roughly $16 to $19 to your Medicare reimbursement depending on your geographic location.
G2211 is an add-on code, which means you can never bill it alone. It must accompany specific office visit codes for established patients (99211-99215) or certain other outpatient E/M codes. When billed correctly, it adds roughly $16 to $19 to your Medicare reimbursement depending on your geographic location.
The code recognizes that some providers serve as the main coordinator of a patient’s care. They track multiple conditions, adjust treatments based on how different medications interact, coordinate with specialists, and maintain continuity over time. This work happens during regular office visits but requires more thought, planning, and follow-up than standard episodic care.
Think of it this way. A walk-in clinic sees a patient once for an upper respiratory infection, treats it, and doesn’t expect to see that patient again for that problem. That’s episodic care. Your primary care doctor sees you regularly for diabetes, hypertension, and high cholesterol, adjusts your medications quarterly, monitors your lab results, and refers you to specialists when needed. That ongoing coordination justifies G2211.
The code isn’t about the length or level of the office visit. It’s about the relationship and responsibility the provider has for the patient’s ongoing care. You can bill a level 2 or level 5 E/M visit with G2211, as long as the visit meets the criteria for ongoing care coordination.
When You Should Use G2211
CMS describes three main scenarios where G2211 applies:
- The first involves providers who serve as the central point of care for a patient with a serious condition. This might be an oncologist managing a cancer patient’s treatment, a cardiologist overseeing heart failure care, or a rheumatologist coordinating lupus management. The key is that you’re the primary provider for that significant condition, not just consulting occasionally.
- The second scenario covers patients with multiple chronic conditions where you’re managing several issues simultaneously. A primary care provider seeing a patient with diabetes, COPD, and chronic kidney disease would fit this category. You’re not just treating one problem at a time. You’re considering how each condition affects the others and adjusting care accordingly.
- The third scenario involves care coordination across multiple providers or settings. When you’re the physician pulling together information from specialists, monitoring hospital discharge plans, and ensuring continuity across the care team, that coordination work supports G2211 billing.
In all these cases, the relationship extends beyond the current visit. You expect to see this patient again. You’re tracking their progress over time. You’re making ongoing adjustments to their care based on how they respond to treatment. This longitudinal responsibility distinguishes G2211-eligible visits from standard episodic care.
When You Cannot Use G2211

Single visits for acute problems don’t qualify, even if the problem seems serious. A patient comes to the emergency department with chest pain, you evaluate them, determine they’re having a heart attack, and admit them to the hospital. That’s serious and requires significant work, but it’s not ongoing care. G2211 doesn’t apply to emergency department visits anyway, but the principle matters. One-time evaluations, even for serious conditions, don’t meet the ongoing care requirement.
Consultations where another provider maintains primary responsibility also don’t qualify. An endocrinologist sees a patient one time at a primary care doctor’s request to evaluate thyroid function and provide recommendations. The endocrinologist isn’t taking on ongoing care. They’re offering expert advice and sending the patient back to the referring provider. That consultation shouldn’t include G2211.
New patient visits create a gray area. Some practices bill G2211 on initial visits when they’re taking over ongoing care from another provider or establishing a new care relationship for serious conditions. Others wait until the second visit when the ongoing relationship is clearly established. CMS hasn’t provided definitive guidance here, so practices need to make reasonable decisions based on the spirit of the code.
Routine follow-up visits that don’t involve serious conditions or multiple chronic problems shouldn’t automatically get G2211. A patient comes in every six months for a blood pressure check, their pressure is controlled on current medication, and no adjustments are needed. While you’re providing ongoing care in a general sense, this routine monitoring of a single well-controlled condition likely doesn’t meet the threshold for G2211.
Billing G2211 Correctly
G2211 only pairs with specific E/M codes. For most practices, this means established patient office visits (99211-99215). It can also pair with certain home visit codes, domiciliary care codes, and nursing facility visit codes. Check the Medicare Physician Fee Schedule to confirm which codes are valid combinations.
You cannot bill G2211 with new patient visits (99202-99205), preventive visits (99381-99397), or annual wellness visits (G0438-G0439). The code applies specifically to problem-focused ongoing care, not initial evaluations or wellness services.
Here’s what proper billing looks like:
- Line one: E/M code (for example, 99214)
- Line two: G2211 (no modifier needed in most cases)
- Both lines should have the same date of service
- Diagnosis codes should reflect the serious or multiple chronic conditions
Documentation must support both the E/M level you’re billing and the use of G2211. For the E/M code, you need the standard history, examination, and medical decision-making elements based on current E/M guidelines. For G2211, your note should reflect ongoing care coordination. Document that you’re managing serious conditions or multiple chronic problems, that you’re coordinating with other providers when applicable, and that you expect continued follow-up.
Many practices add a brief statement to their documentation templates: “Provider serves as primary coordinator for patient’s ongoing care of [condition(s)].” While not strictly required, this type of statement helps demonstrate that you’re consciously applying G2211 based on the patient relationship, not just adding it automatically to every visit.
G2211 and Modifier 25 Rules
Modifier 25 issues with G2211 changed between 2024 and 2025, creating confusion for practices that had just figured out the 2024 rules. Initially, CMS required Modifier 25 on G2211 when billed with a procedure on the same day. Starting January 1, 2025, CMS changed this policy. You no longer append Modifier 25 to G2211, even when billing it with same-day procedures.
Here’s how it works now. You see an established patient for ongoing diabetes management. During the visit, you also remove a skin tag.
You bill:
- 99214-25 (E/M with Modifier 25)
- G2211 (no modifier)
- 11200 (skin tag removal, no modifier)
The Modifier 25 goes on the E/M code to show it was separately identifiable from the procedure. G2211 tags along with the E/M code without needing its own modifier. This makes logical sense since G2211 is an add-on code describing characteristics of the E/M service rather than a standalone service itself.
The 2024-2025 modifier rule change illustrates a broader issue with G2211. The guidance keeps shifting as CMS responds to questions and confusion from the field. This means practices need to stay current with Medicare updates and be ready to adjust their billing practices when policies change.
Documentation That Supports G2211
 Your medical record should make it obvious why G2211 applies without requiring an auditor to read between the lines. Document the conditions you’re managing, especially if they’re multiple or serious. Note coordination activities like reviewing specialist reports, discussing care with other providers, or adjusting treatments based on information from other sources.
Your medical record should make it obvious why G2211 applies without requiring an auditor to read between the lines. Document the conditions you’re managing, especially if they’re multiple or serious. Note coordination activities like reviewing specialist reports, discussing care with other providers, or adjusting treatments based on information from other sources.
Many electronic health record systems now include G2211 prompts or checkboxes. While these can be helpful reminders, don’t rely on checking a box to meet documentation requirements. The actual note content should reflect ongoing care coordination. Describe what you’re managing, how conditions interact, what you’re monitoring over time, and what your ongoing care plan includes.
For patients with multiple chronic conditions, list them and explain how you’re managing them together. For example: “Patient’s diabetes management requires careful monitoring given concurrent CKD stage 3 and heart failure. Adjusted metformin dose based on recent eGFR. Monitoring fluid status closely given cardiac and renal issues.”
For patients with single serious conditions, document the ongoing management and coordination required. For example: “Continue to serve as primary coordinator for patient’s stage 3 lung cancer treatment. Reviewed oncology visit notes from last week. Managed nausea related to chemotherapy. Coordinated with oncology regarding dose adjustments.”
Template language can help ensure you’re consistently documenting elements that support G2211, but avoid identical copy-paste language on every visit. Each note should reflect what actually happened during that specific encounter.
Compliance Risks You Need to Know
G2211 is still new enough that audit patterns haven’t fully emerged, but certain red flags will likely attract scrutiny. Using G2211 on every single established patient visit suggests you’re not applying clinical judgment about when ongoing care coordination actually occurs. A more realistic pattern shows G2211 on most visits for your chronically ill patients but not on every brief recheck or minor acute problem.
Billing G2211 on visits that don’t involve serious or chronic conditions raises questions. If your documentation shows a patient came in for a minor rash that you treated and don’t expect to see again, G2211 doesn’t fit even if the patient has other chronic conditions that weren’t addressed during this visit.
Practices should conduct regular internal audits of G2211 usage. Pull a sample of claims with the code and review the documentation. Does it support ongoing care coordination? Is there evidence of serious or multiple chronic conditions? Would an external auditor agree that G2211 was appropriate based on the note?
Staff education is critical because G2211 requires clinical judgment that goes beyond simple coding rules. Billers and coders need to recognize when documentation supports the code. Providers need to create documentation that accurately reflects the care they provide. Front office staff should schedule patients appropriately so visits intended for ongoing care management aren’t rushed through limited appointment slots.
Financial Impact on Your Practice
 For a practice seeing a significant number of Medicare patients with chronic conditions, G2211 represents meaningful additional revenue. A primary care practice billing G2211 on 40% of their established patient visits might see $50,000 to $100,000 in additional annual Medicare payments. The exact amount depends on visit volume, geographic location, and specialty.
For a practice seeing a significant number of Medicare patients with chronic conditions, G2211 represents meaningful additional revenue. A primary care practice billing G2211 on 40% of their established patient visits might see $50,000 to $100,000 in additional annual Medicare payments. The exact amount depends on visit volume, geographic location, and specialty.
However, this revenue only materializes when you bill the code correctly and consistently. Many practices are still underutilizing G2211 because of uncertainty about when it applies. They’re leaving money on the table for legitimate ongoing care coordination work.
The flip side is that overbilling G2211 creates financial risk. If auditors determine you’re using the code inappropriately, you’ll need to refund payments plus potentially face penalties. Getting clear policies in place now prevents expensive problems later.
G2211 also aligns with broader healthcare payment trends toward recognizing care coordination and continuity. As Medicare and other payers move toward value-based payment models, codes like G2211 that reward longitudinal care relationships become increasingly important. Practices that build strong chronic disease management programs position themselves well for both current G2211 payment and future value-based arrangements.
Making G2211 Work in Your Practice
Start by identifying which patient populations in your practice clearly qualify for G2211. Create profiles of typical patients who meet the criteria. For primary care, this might include patients with three or more chronic conditions or patients with single serious conditions like cancer, heart failure, or COPD where you serve as the care coordinator.
Develop internal guidelines that give your billing staff clear direction on when G2211 applies. Include specific examples from your specialty and patient mix. Train providers on documentation requirements and give them tools like templates or note prompts that remind them to document ongoing care coordination.
Consider creating a G2211 workflow that flags appropriate patients during scheduling or check-in. When a patient with multiple chronic conditions books a follow-up visit, your system can alert staff that this visit likely qualifies for G2211. This helps ensure you’re capturing the code consistently without adding it inappropriately to acute visits.
Monitor your G2211 usage rates and denial patterns. Track what percentage of established patient visits include G2211 and compare this to your patient mix. Are you using it too frequently? Not often enough? Do certain payers deny it more than others? This data helps you refine your approach and identify training needs.
Find Expert Reimbursement Support
![]() G2211 represents just one of many billing challenges that practices face. Between new codes, changing modifier rules, varying payer policies, and documentation requirements, keeping up with billing best practices demands significant time and expertise. Many practices find that professional billing support delivers better results with less stress.
G2211 represents just one of many billing challenges that practices face. Between new codes, changing modifier rules, varying payer policies, and documentation requirements, keeping up with billing best practices demands significant time and expertise. Many practices find that professional billing support delivers better results with less stress.
At Medwave, our billing team stays current with Medicare updates including G2211 guidance changes. We help practices develop appropriate use policies, train staff on correct implementation, and audit G2211 usage to ensure compliance while maximizing legitimate reimbursement.
Because we handle billing, credentialing, and payer contracting together, we see how these functions connect. We ensure your providers are credentialed correctly with Medicare to bill G2211. We help you negotiate appropriate rates for your services in payer contracts. We make sure billing practices align with contract terms and regulatory requirements.
Our clients report fewer denied claims, faster payment cycles, and reduced audit risk when we manage their billing. We conduct regular reviews of new codes like G2211, provide documentation feedback to providers, and help practices adapt quickly when CMS changes policies.
If you’re uncertain about your G2211 usage, concerned about compliance risks, or simply want to ensure you’re capturing all available revenue, contact Medwave for a free billing assessment. We’ll review your current approach to G2211, identify opportunities for improvement, and show you how professional billing support benefits your practice.
G2211 doesn’t have to be confusing or risky. With clear policies, solid documentation, appropriate training, and attention to CMS guidance, you can use this code confidently to receive fair payment for the ongoing care coordination work you provide every day. The key is building systems that ensure consistent, appropriate use while maintaining the documentation necessary to support your claims.