There’s a particular kind of frustration that comes with completing the credentialing process, submitting all the right paperwork, waiting through the review period, and then finding out the payer panel is closed. You did everything right, and you still can’t see those patients in-network. It’s one of the more discouraging moments a provider or practice administrator can face, and it happens more often than most people realize.
The good news is that a closed panel is not necessarily a permanent wall. It’s an obstacle, and like most obstacles in healthcare administration, it responds better to strategy than to frustration. This article walks you through what closed payer panels actually are, why payers close them, how to find out a panel’s status before you waste time applying, and what you can realistically do to get in even when the door appears to be shut.
What is a Closed Payer Panel?
 A payer panel is the network of credentialed providers that a health plan uses to deliver care to its members. When a patient has insurance with a particular plan and sees an in-network provider, that provider is on the plan’s panel. Being on the panel means you’ve been credentialed, you’ve signed a contract, and the payer will reimburse you at the negotiated in-network rate.
A payer panel is the network of credentialed providers that a health plan uses to deliver care to its members. When a patient has insurance with a particular plan and sees an in-network provider, that provider is on the plan’s panel. Being on the panel means you’ve been credentialed, you’ve signed a contract, and the payer will reimburse you at the negotiated in-network rate.
A closed panel means the payer is not currently accepting new in-network providers. This can apply across an entire plan, or it can be limited to a specific specialty, geographic area, or plan type. The payer has determined that it has enough providers in that category to meet its network needs, and it’s not looking to add more right now.
It’s worth being clear about what a closed panel is not. It is not a credentialing denial. A denial means the payer reviewed your application and found a reason not to credential you. A closed panel means the payer isn’t accepting anyone new in your category, regardless of qualifications. The distinction matters because the response to each situation is completely different.
Panels also exist on a spectrum. Some are fully open, meaning the payer is actively recruiting new providers. Some are fully closed. And some are partially open, meaning the payer is accepting new providers in certain specialties or zip codes but not others. A plan might be closed to new primary care physicians in a major metro area but still accepting specialists in rural counties nearby. This is why checking panel status requires more than a yes or no question.
Why Payers Close Their Panels
Payers close panels for reasons that make sense from a business standpoint, even when they’re deeply inconvenient for providers. The most common reason is network saturation. Every payer has to maintain what’s called network adequacy, which means having enough providers of each type in each geographic area to give members reasonable access to care. CMS sets specific network adequacy standards for Medicare Advantage plans, and state regulators set similar requirements for Medicaid and commercial plans.
Once a payer determines that its network meets adequacy standards in a given area and specialty, it has little incentive to keep adding providers. In fact, adding more providers can increase utilization and drive up plan costs. Narrow networks, which limit the number of in-network providers, are one of the tools payers use to keep premiums competitive. When a plan’s network is already meeting the required standards, opening the panel doesn’t benefit the payer financially.
Cost control is the other major driver. More providers in a network generally means more utilization, which means more claims paid. In markets where payers are competing aggressively on premium price, keeping the network lean is part of the financial model. This is especially true for HMO and EPO plan types, where members are required to stay in-network for coverage. PPO networks tend to be broader and close less frequently, while HMO panels can close quickly once geographic coverage targets are met.
There’s also a category of panel closure that isn’t formal at all. Some payers become so backlogged in their credentialing departments that they stop accepting new applications simply because they don’t have the capacity to process them. This can look identical to a formal panel closure from the outside, but it’s actually a temporary administrative situation. Knowing the difference matters because the approach to resolving each one is different.
How Closed Panels Hurt Your Practice
 The financial impact of a closed panel is direct and measurable. When you’re out of network with a major payer in your area, patients covered by that plan face higher out-of-pocket costs to see you. Some of them will choose not to. Others will never find you in the first place because you won’t appear in the payer’s provider directory. For a new practice or a provider expanding into a new market, missing a key payer can significantly slow patient volume growth.
The financial impact of a closed panel is direct and measurable. When you’re out of network with a major payer in your area, patients covered by that plan face higher out-of-pocket costs to see you. Some of them will choose not to. Others will never find you in the first place because you won’t appear in the payer’s provider directory. For a new practice or a provider expanding into a new market, missing a key payer can significantly slow patient volume growth.
The referral implications are just as significant. If the dominant hospital system or the largest primary care group in your area uses a particular plan heavily, not being on that panel can effectively cut you off from their referral network. Specialists feel this acutely. A cardiologist who isn’t on the same plan as the referring primary care physicians in the area will simply stop getting those referrals, not because of anything related to clinical quality, but because the insurance doesn’t work.
Here’s what makes this particularly painful for small and independent practices: the problem often surfaces too late. A provider signs a lease, hires staff, builds out a schedule, and then discovers during the credentialing process that a key payer’s panel has been closed for months. The credentialing timeline already runs 90 to 120 days for most payers under normal circumstances. Finding out at the end of that process that the panel is closed is a costly surprise that could have been avoided with earlier research.
How to Check Panel Status Before You Apply
This is a step that saves practices significant time and money, and it’s one that gets skipped far too often.
The most direct approach is calling the payer’s provider relations line and asking specifically whether the panel is open for your specialty and your practice location. Ask for that confirmation in writing if at all possible. Verbal confirmations are useful but not binding, and payer staff can sometimes give outdated or inconsistent information depending on who you reach.
Many larger payers also publish panel availability information through their provider portals, though the accuracy and timeliness of that information varies. A portal might show a panel as open when it’s effectively been closed for months at the operational level. Use portal information as a starting point, not as your only source.
The most reliable approach, especially for practices credentialing with multiple payers simultaneously, is working with a credentialing service that maintains ongoing relationships with payer provider relations departments. A credentialing partner who talks to these payers regularly will often know the real panel status before it’s reflected anywhere publicly. That kind of current, specific knowledge is one of the most practical benefits of working with a credentialing team that specializes in this area.
Strategies for Getting on a Closed Panel
 A closed panel is a starting point for a conversation, not the end of one. Here are the approaches that have the best track record for getting providers into closed networks.
A closed panel is a starting point for a conversation, not the end of one. Here are the approaches that have the best track record for getting providers into closed networks.
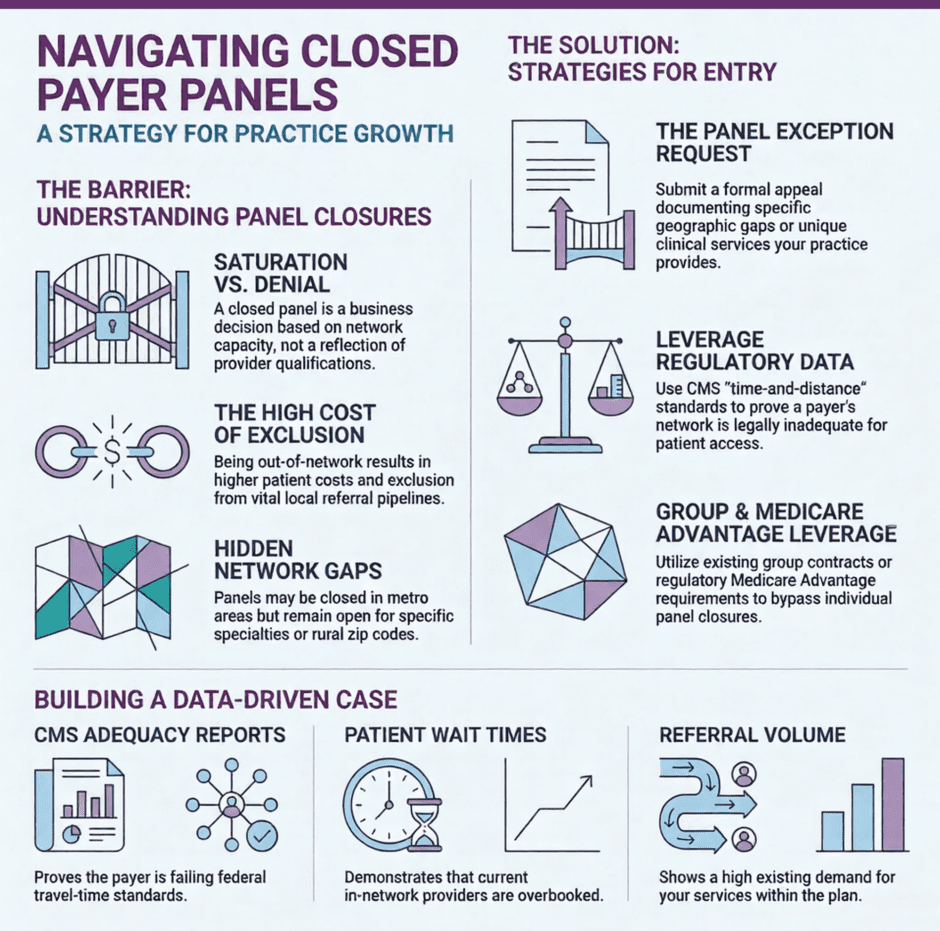
The panel exception request is the most direct tool available. This is a formal letter submitted to the payer requesting that they make an exception to the panel closure and credential your practice. The key to making this work is building a specific, documented case for why the network needs you. Generic requests get ignored. Requests that demonstrate a concrete gap in patient access get read.
Here’s what a strong panel exception request should include:
- A clear description of the geographic or specialty gap you would fill, supported by data from CMS network adequacy reports or state insurance department resources
- Evidence of patient demand, such as referral volume, wait time data, or documented patient requests for an in-network provider of your specialty in your area
- Your clinical credentials, any hospital affiliations, and any unique services you offer that aren’t currently well-represented in the network
Network adequacy data is your friend here. CMS publishes network adequacy standards and compliance data for Medicare Advantage plans, and many state insurance departments publish similar data for Medicaid and commercial plans. If you can show that the payer’s network doesn’t meet the required time-and-distance standards for your specialty in your county, you have a regulatory argument, not just a business request.
Group and hospital affiliations can also open doors that are closed to individual providers. If you’re employed by or affiliated with a health system that already has a contract with the payer, that system’s existing relationship can sometimes be used to add new providers to the panel under the group’s umbrella contract. This is worth exploring before pursuing the exception request route independently.
Medicare Advantage Panels Deserve Special Attention
Medicare Advantage has grown dramatically over the past decade, and it now represents a significant share of the patient population for most practices. At the same time, MA plans are among the most aggressive about closing panels once network adequacy standards are met.
CMS sets specific time and distance standards for Medicare Advantage networks, broken down by specialty and geography. These standards specify how far a beneficiary should have to travel to access a particular type of provider. If a plan’s network doesn’t meet those standards, CMS can require the plan to add providers. That’s a regulatory mechanism that providers can use to support a panel exception request.
The stakes of being outside MA networks are growing as enrollment continues to rise. In many markets, Medicare Advantage now covers more Medicare beneficiaries than traditional fee-for-service Medicare. A practice that isn’t credentialed with the major MA plans in its area is effectively locked out of a large and growing portion of the Medicare population.
Staying Ready When Panels Reopen
 Panels don’t stay closed forever. Payers periodically reopen panels when membership grows, when existing network providers retire or relocate, or when CMS or state regulators require network expansions to meet adequacy standards. The problem is that payers don’t always make formal public announcements when this happens.
Panels don’t stay closed forever. Payers periodically reopen panels when membership grows, when existing network providers retire or relocate, or when CMS or state regulators require network expansions to meet adequacy standards. The problem is that payers don’t always make formal public announcements when this happens.
Practices that are positioned to apply the moment a panel reopens have a significant advantage over those who are starting from scratch. Maintaining a relationship with the payer’s provider relations team, even while the panel is closed, is one of the most effective ways to get that early notice. A brief, professional check-in every few months keeps your name in the conversation without being a nuisance.
Keeping your CAQH profile current matters here too. When a panel reopens and a payer starts processing applications, providers with complete and current CAQH profiles move through the process faster. An outdated profile is a simple and avoidable reason to fall behind in a credentialing queue.
FAQs
- What does it mean when a payer panel is closed?
It means the payer is not currently accepting new in-network providers for a specific specialty, geography, or plan type. It is not a denial of your application. It means the payer has determined its network is adequately staffed for now. - Can I still see patients if a payer panel is closed?
You can see patients who are covered by that plan, but you’ll be out of network. Patients will typically pay higher cost-sharing, and you won’t be reimbursed at the contracted in-network rate. Some patients will choose other providers as a result. - What is a panel exception request?
It’s a formal letter submitted to the payer requesting that they credential you despite the panel closure. The strongest requests include specific documentation of a patient access gap or network adequacy issue that your practice would help address. - How long do panels stay closed?
It varies significantly by payer and market. Some panels reopen within a few months when membership grows or providers leave the network. Others stay closed for a year or more. There’s no standard timeline. - Does being part of a group practice help?
Yes, in some cases. If the group already has a contract with the payer, adding a new provider under an existing group agreement can sometimes bypass individual panel closures. This depends on the payer’s policies and the structure of the existing contract. - Can a credentialing service help with a closed panel?
Absolutely. An experienced credentialing partner will know current panel status across major payers, have relationships with provider relations teams, and have experience preparing exception requests that are framed in a way that actually gets reviewed seriously.
Summary: Tackling Closed Payer Panels
![]() A closed payer panel is frustrating, but it’s not the end of the road. With the right information, the right timing, and a well-prepared exception request, providers get into closed networks regularly. The key is approaching it strategically rather than assuming the answer is final.
A closed payer panel is frustrating, but it’s not the end of the road. With the right information, the right timing, and a well-prepared exception request, providers get into closed networks regularly. The key is approaching it strategically rather than assuming the answer is final.
At Medwave, we work with practices on credentialing, billing, and payer contracting, and closed panels are something we deal with on a regular basis. We know which panels are open in which markets, we have relationships with payer provider relations teams, and we know how to build an exception request that makes a genuine case for network inclusion. If a closed panel is standing between your practice and the patients you want to serve, reach out to us. Let’s figure out the best path forward together.