
If you’ve ever managed physician credentialing, you already know how much time primary source verification can eat up. You’re bouncing between state licensing board websites, waiting on fax confirmations, manually entering data into spreadsheets, and hoping nothing falls through the cracks before a deadline hits. It’s tedious work, and the margin for error is higher than most organizations are comfortable admitting.
 Primary source verification, or PSV, is the process of confirming a provider’s credentials directly from the original issuing authority. That means going to the actual licensing board, the actual medical school, the actual training program, rather than relying on copies a provider submits. It’s a requirement for accreditation bodies like The Joint Commission, NCQA, and DNV, and it’s a fundamental piece of patient safety. But the way most organizations have been doing it for years is no longer holding up under the current volume and pace demands of healthcare.
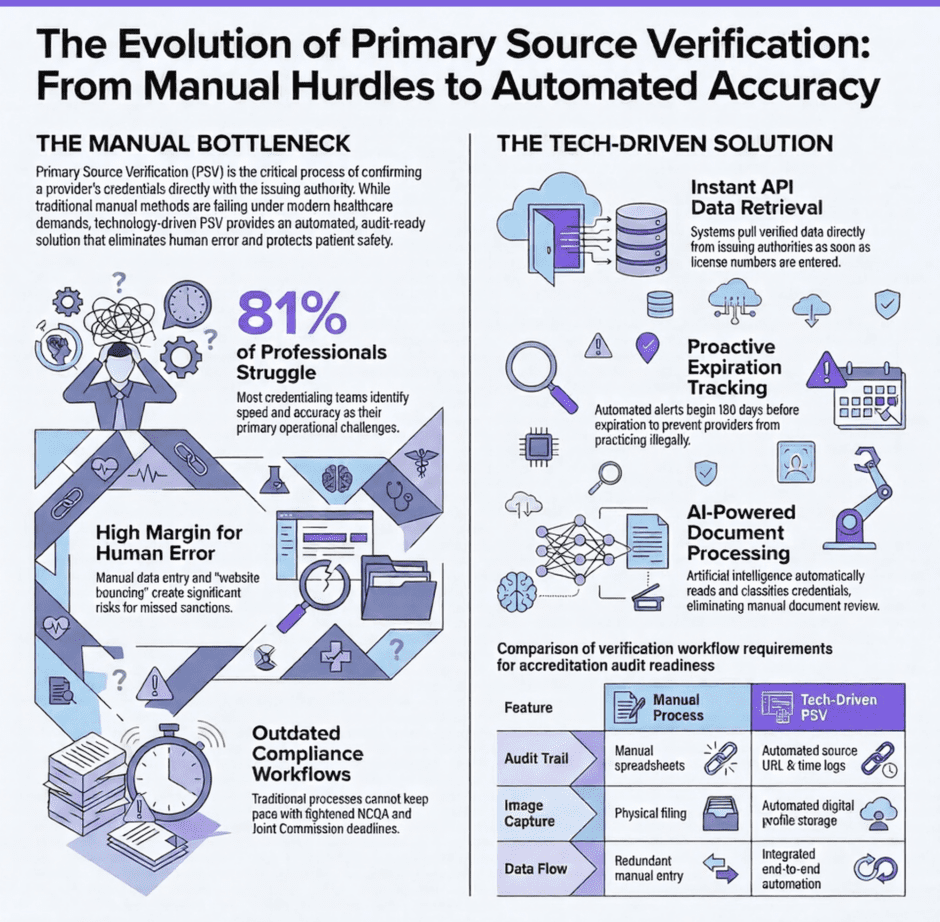
Primary source verification, or PSV, is the process of confirming a provider’s credentials directly from the original issuing authority. That means going to the actual licensing board, the actual medical school, the actual training program, rather than relying on copies a provider submits. It’s a requirement for accreditation bodies like The Joint Commission, NCQA, and DNV, and it’s a fundamental piece of patient safety. But the way most organizations have been doing it for years is no longer holding up under the current volume and pace demands of healthcare.
Technology is changing that. Not in a vague, futuristic way, but in practical, immediate ways that credentialing teams are already using to work faster, make fewer mistakes, and stay ahead of compliance deadlines. This article breaks down what that looks like and why it matters for every organization that credentials physicians.
Why the Old Way of Doing PSV Isn’t Working Anymore
The traditional PSV process was built for a simpler time. A credentialing specialist would receive a provider’s application, pull together the relevant license information, contact each issuing authority individually, wait for responses, document what came back, and file everything in a physical or digital folder. That process worked when provider volume was manageable and licensing was mostly confined to a single state.
That’s not the world most credentialing teams are operating in today. The number of licensed healthcare professionals has grown significantly, and many providers hold licenses in multiple states, carry several certifications, and operate across different practice settings simultaneously. Each one of those credentials needs to be verified at the primary source, tracked for expiration, and re-verified on a regular cycle.
According to a 2025 poll conducted by MedTrainer, 81 percent of credentialing professionals identify speed and accuracy as their top challenges. That’s not a staffing problem. That’s a process problem. Manual workflows that require a person to visit each state board website individually, download documents, re-upload them, and manually enter data into a system were never designed for the scale that credentialing teams are dealing with now.
There’s also a compliance dimension that has become more urgent. NCQA tightened its verification deadlines in recent years, and the penalties for credentialing failures, whether a lapsed license or a missed sanction, fall directly on the organization. Fraud and credential misrepresentation are real risks in healthcare, and the consequences of credentialing someone who shouldn’t be practicing are serious. The manual process that relied on individual staff members to catch every problem is simply not reliable enough given what’s at stake.
What Technology-Driven PSV Actually Does Differently
The core difference between manual PSV and technology-driven PSV is where human judgment gets applied. In a manual process, staff spend most of their time on data retrieval tasks: navigating to websites, waiting for results, typing information into fields, saving documents to the right folders. These are tasks that don’t require professional judgment. They just require time and attention, and they’re exactly the kind of tasks that automation handles well.
When PSV technology is working correctly, it retrieves license verification data directly from the issuing authority the moment a provider’s license number is entered into the system. The relevant fields get populated automatically, reducing the risk of typos or data entry errors. The license image is captured and stored in the provider’s digital profile. A trusted URL is logged alongside the verification, so there’s a clear audit trail showing exactly where the information came from and when it was retrieved.
That audit trail matters more than it might seem. Accreditation bodies don’t just want to know that you verified a provider’s license. They want to know that you verified it at the primary source, that you documented the process, and that you can produce that documentation on demand. A technology platform that automatically logs the source URL, the date of verification, and the name of the person who confirmed it creates exactly the kind of record that auditors and accreditation reviewers are looking for.
The Features That Separate Effective PSV Technology from the Rest
Not all PSV technology delivers the same value. When evaluating what your organization needs, there are a few features that make the difference between a system that genuinely improves your process and one that just adds another platform to manage.
The first is on-demand automation that triggers as soon as a license number is entered. You shouldn’t have to initiate a separate verification request or wait for a batch process to run overnight. The system should begin retrieving data immediately, and it should populate the relevant fields in the provider’s profile without requiring manual re-entry. Look for platforms that offer unlimited verifications without additional per-transaction costs, since artificial usage caps create incentives to skip verifications or delay them.
Coverage is the second critical factor. A PSV platform that only verifies DEA registrations and a handful of state licenses will create gaps in your process that you’ll have to fill manually. You need coverage across all license types in all states, including nursing licenses, advanced practice credentials, and specialty certifications, not just physician licenses. As your organization grows and adds providers with more varied licensing profiles, your PSV technology needs to grow with it.
The third feature worth prioritizing is direct integration with the original issuing source through an API connection. When the system accesses license data directly from the state board through an official connection, you get accurate, current data rather than information that may have passed through an intermediary and become outdated. Direct API access also tends to be more reliable and less vulnerable to disruptions caused by website changes or access restrictions at the source.
Here are the other features that round out a genuinely effective PSV platform:
- Automated expiration reminders that begin well in advance of the renewal date, ideally starting four to six months out, with notifications going to both the credentialing team and the provider directly
- Image capture functionality that pulls the actual license document into the provider’s profile, which is specifically required for Joint Commission and DNV accreditation
- Integration with broader credentialing workflows so that verified license data flows automatically into credentialing packets, enrollment applications, and privilege requests without needing to be re-entered
Expiration Tracking: The Part of PSV That Keeps Practices Up at Night
 License expirations are one of the most common and most preventable credentialing failures. A provider whose license lapses can’t legally practice, and an organization that allows a provider to see patients on an expired license faces real liability exposure. The problem isn’t that credentialing teams don’t know this. It’s that tracking dozens or hundreds of expiration dates across multiple providers, license types, and states is genuinely hard to do without automated support.
License expirations are one of the most common and most preventable credentialing failures. A provider whose license lapses can’t legally practice, and an organization that allows a provider to see patients on an expired license faces real liability exposure. The problem isn’t that credentialing teams don’t know this. It’s that tracking dozens or hundreds of expiration dates across multiple providers, license types, and states is genuinely hard to do without automated support.
Manual expiration tracking usually means a spreadsheet with color coding and someone checking it regularly and sending reminder emails one at a time. That process is only as reliable as the person maintaining it. When that person is out sick, handling a credentialing surge, or simply overlooked updating the spreadsheet, licenses slip through.
Automated expiration tracking changes the dynamic entirely. When a license is added to the system with an expiration date, the platform takes responsibility for monitoring it and sending reminders on a set schedule. Reminders go out at 180 days, 120 days, 90 days, or whatever intervals make sense for your organization. They go to the credentialing team and to the provider, so the burden of renewal awareness doesn’t sit entirely on the administrative side. Reports can be filtered and sorted by upcoming expiration dates, giving credentialing managers a real-time view of what needs attention and when.
This kind of proactive monitoring is also a requirement under NCQA’s updated credentialing standards. The ability to pull a report showing all licenses with upcoming expirations, sorted by date, isn’t just operationally useful. It’s a compliance necessity.
How PSV Technology Fits Into the Broader Credentialing Workflow
One of the most significant benefits of modern PSV technology is that it doesn’t have to live in isolation. When PSV is integrated into a broader credentialing platform, verified license data flows directly into other workflows without requiring manual intervention.
Here’s what that integration looks like in practical terms:
- A new provider is added to the system and their license number is entered. The platform retrieves verification data from the state board, captures the license image, logs the source URL, and populates the provider’s digital profile automatically.
- Because the license has been added as a required document in the credentialing packet template, the platform automatically pulls the verified license into the packet. The packet status updates to reflect the new document, so the credentialing specialist doesn’t have to manually confirm that each piece is in place.
- When the provider enrolls with a payer or applies for hospital privileges, the license data that was already verified and stored in the profile can be pulled directly into those applications, eliminating redundant data entry across multiple processes.
That kind of end-to-end flow reduces the time credentialing staff spend on repetitive tasks and significantly reduces the risk of data inconsistencies across different parts of the credentialing record. When the same license information is entered manually in four different places, there are four opportunities for a typo or an outdated entry to create a problem. When it’s entered once and flows automatically, that risk disappears.
AI Is Starting to Play a Real Role in PSV
 Automation handles the retrieval and routing of data well, but the next frontier in credentialing technology is using artificial intelligence to handle the document-heavy parts of the process that have traditionally required human eyes and hands.
Automation handles the retrieval and routing of data well, but the next frontier in credentialing technology is using artificial intelligence to handle the document-heavy parts of the process that have traditionally required human eyes and hands.
AI-powered document upload tools can now read a provider’s credential documents, classify them by type, extract key data points like names, license numbers, and expiration dates, and place them in the correct location within the provider’s digital profile, all within seconds of the document being uploaded. This eliminates the manual document review step that used to require a staff member to open each file, read it, and manually enter the relevant information.
The practical impact of this is substantial. During a large provider onboarding, when dozens of documents may come in at once, AI-assisted processing means the entire batch can be handled in the time it used to take to process a handful of records manually. Every expiration date gets captured, every file ends up in the right place, and every provider profile stays current without requiring proportional increases in staff time.
AI form mapping, which automatically recognizes and fills in fields across long credentialing application forms using data already stored in the provider’s profile, is another capability that’s moving from concept to reality. Credentialing forms are notoriously long and repetitive, often asking for the same information in slightly different formats across dozens of pages. Automating that process doesn’t just save time. It reduces the fatigue-related errors that come from staff manually completing the same information over and over again.
What This Means for Patient Safety
It’s easy to frame PSV technology as an efficiency story, and the efficiency gains are real and significant. But the more important story is about patient safety.
Primary source verification exists because patients have a right to know that the person treating them is who they say they are, holds the credentials they claim to hold, and is in good standing with their licensing authority. When PSV is done manually and inconsistently, gaps happen. Licenses get missed. Sanctions don’t get caught. Providers practice on expired credentials because no one had time to follow up on the renewal reminder.
Technology doesn’t eliminate the need for human judgment in credentialing. Someone still needs to review what the system retrieves, confirm that it makes sense, and make decisions when something looks off. But technology can dramatically reduce the risk that a verification gets skipped entirely, that an expiration slips by unnoticed, or that a sanction goes unchecked because the manual monitoring process didn’t catch it in time. That’s not just an operational improvement. It’s a patient safety improvement.
FAQs
- What is primary source verification for physicians?
Primary source verification is the process of confirming a physician’s credentials directly with the original issuing authority, such as a state medical board, medical school, or training program. It’s required by accreditation bodies including The Joint Commission, NCQA, and DNV. - Why is manual PSV a problem for healthcare organizations?
Manual PSV requires staff to visit multiple websites, wait for responses, manually enter data, and track expiration dates across numerous providers. As provider volume grows and licensing becomes more multi-state, the manual process becomes slow, error-prone, and difficult to scale. - What does automated PSV technology do?
Automated PSV technology retrieves license verification data directly from issuing authorities as soon as a license number is entered, populates provider profile fields automatically, captures the license image, logs the source URL for the audit trail, and sends automated expiration reminders. - Is image capture required for accreditation?
Yes. The Joint Commission and DNV both require that a copy of the license or credential be captured as part of the PSV process. Not all PSV platforms include image capture, so it’s an important feature to confirm before selecting a vendor. - How does PSV technology support NCQA compliance?
NCQA requires that verifications be performed at the primary source, that expiration dates be tracked and acted upon, and that documentation of the verification process be maintained. Technology platforms that log the source URL, date, and verifying staff member’s name, and that generate reports filtered by expiration date, directly support NCQA audit requirements. - How does PSV integration with credentialing workflows save time?
When PSV is integrated with the broader credentialing platform, verified license data flows automatically into credentialing packets, enrollment applications, and privilege requests. This eliminates redundant data entry and reduces the risk of inconsistencies across different parts of the credentialing record.
Summary: PSV is Being Fixed by Technology
![]() Primary source verification has always been a critical function in healthcare credentialing. What’s changing is how it gets done. The organizations that are seeing the biggest improvements in credentialing speed, accuracy, and compliance are the ones that have moved away from manual, fragmented verification processes and toward technology that handles data retrieval, tracking, and documentation automatically.
Primary source verification has always been a critical function in healthcare credentialing. What’s changing is how it gets done. The organizations that are seeing the biggest improvements in credentialing speed, accuracy, and compliance are the ones that have moved away from manual, fragmented verification processes and toward technology that handles data retrieval, tracking, and documentation automatically.
The efficiency gains are meaningful. The compliance benefits are significant. The patient safety implications are the most important part of the whole picture.
At Medwave, we work with medical practices and healthcare organizations on credentialing, billing, and payer contracting. We know firsthand how much a disorganized or outdated credentialing process can cost an organization, in time, in revenue, and in compliance exposure. If your PSV process is still heavily manual, or if you’re unsure whether your current approach meets accreditation standards, reach out to Medwave. We can help you take a hard look at where the gaps are and what a better process looks like for your specific situation.