
Radiology billing requires precise coding to ensure proper reimbursement for diagnostic imaging services. Running a standalone imaging center or providing radiology services as part of a larger healthcare practice can be challenging. So, knowing which CPT codes to use makes all the difference between getting paid promptly and facing claim denials. This guide walks you through the essential CPT codes used in radiology billing, helping you bill accurately and maximize your revenue.
What Are Radiology CPT Codes?
 CPT codes , or Current Procedural Terminology codes, are standardized numerical identifiers developed by the American Medical Association. These codes describe medical procedures and services so that healthcare providers, insurance companies, and Medicare can communicate clearly about what services were performed.
CPT codes , or Current Procedural Terminology codes, are standardized numerical identifiers developed by the American Medical Association. These codes describe medical procedures and services so that healthcare providers, insurance companies, and Medicare can communicate clearly about what services were performed.
In radiology, CPT codes specifically identify imaging procedures and diagnostic tests. The radiology section of CPT codes spans from 70010 to 79999, covering everything from simple X-rays to advanced MRI scans and radiation therapy treatments. Each code represents a specific procedure, the body part being examined, and the type of imaging technology used during the patient’s visit.
Think of these codes as the universal language between your practice and the payers. When you submit a claim with the correct radiology CPT code, the insurance company knows exactly what service you provided, why it was medically necessary, and how much you should be reimbursed.
How Are Radiology CPT Codes Organized?
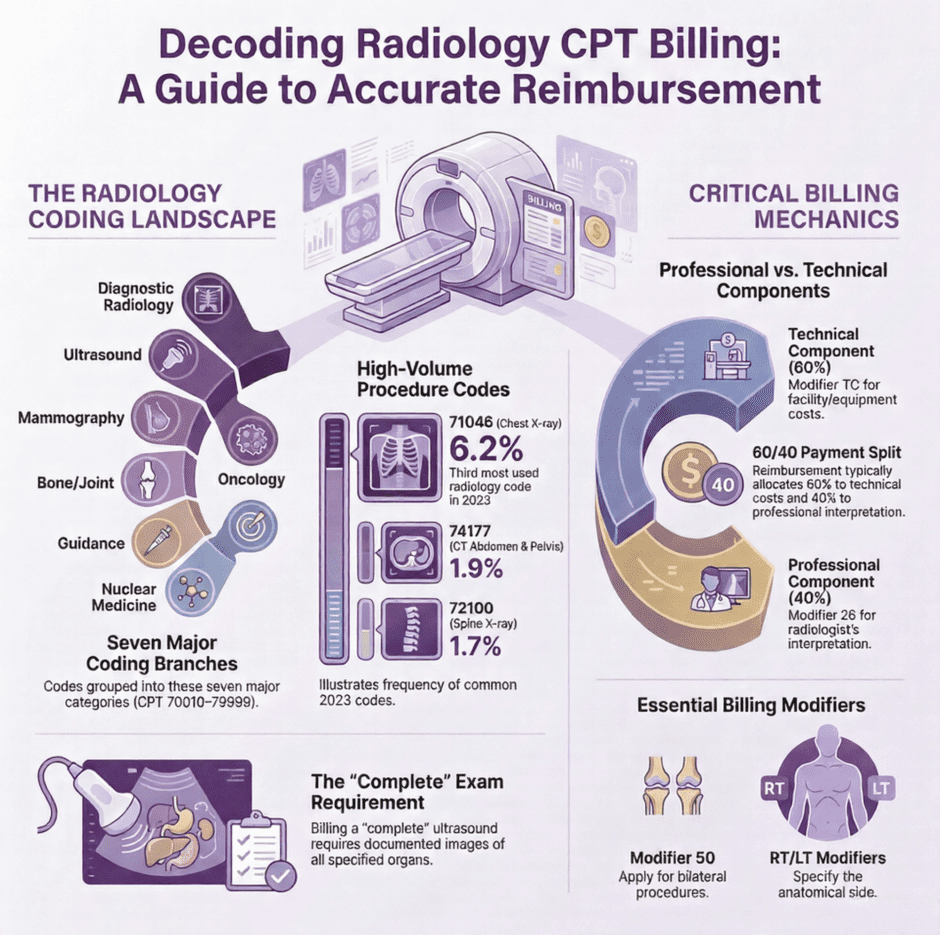
Radiology codes break down into seven main categories, each covering different types of imaging services.
Here’s how the code ranges are structured:
- Diagnostic Radiology (70010-76499): This largest category includes X-rays, CT scans, and MRIs of various body regions. These codes cover the procedures most radiology practices use daily.
- Diagnostic Ultrasound (76506-76999): These codes apply to ultrasound procedures, which use high-frequency sound waves to create images of internal organs and tissues. Common examples include abdominal ultrasounds, pregnancy monitoring, and vascular studies.
- Radiologic Guidance (77001-77022): When imaging helps guide other procedures, such as biopsies or injections, these codes come into play. They’re often used alongside surgical or interventional procedure codes.
- Mammography (77046-77067): Breast imaging has its own dedicated code range. These codes distinguish between screening mammograms and diagnostic mammograms, as well as bilateral and unilateral procedures.
- Bone and Joint Studies (77071-77086): These codes specifically cover imaging focused on bones and joints, including bone density scans and specialized joint studies.
- Radiation Oncology (77261-77799): Cancer treatment procedures using radiation fall under this category. These codes cover treatment planning, radiation delivery, and follow-up care for oncology patients.
- Nuclear Medicine (78012-79999): Procedures involving radioactive materials for both diagnostic and therapeutic purposes use these codes. Examples include bone scans, cardiac stress tests, and thyroid studies.
What Are the Most Common Radiology CPT Codes?
While there are hundreds of radiology codes, certain procedures happen far more frequently than others. Knowing these common codes helps streamline your billing process and reduces errors.
CPT 71046
71046 covers chest X-rays with at least two views. This code was the third most commonly used radiology code in 2023, reported 6.2% of the time at imaging centers nationwide. Providers use this for diagnosing respiratory conditions, checking for pneumonia, evaluating chest pain, and assessing the heart and lungs.
CPT 71045
71045 represents chest X-rays with a single frontal view. This simpler version of the chest X-ray is another high-volume code, often used for routine screenings and follow-up visits.
CPT 72100
72100 bills for radiologic examination of the lumbosacral spine, typically capturing two or three views of the lower back. This code was used 1.7% of the time in 2023 and helps diagnose back injuries, chronic lower back pain, and spinal conditions.
CPT 72148
72148 covers MRI of the lumbar spinal canal without contrast material. As back pain remains one of the most common patient complaints, this code sees frequent use for evaluating disc problems, spinal stenosis, and nerve compression.
CPT 74177
74177 applies when performing a CT scan of the abdomen and pelvis without contrast. This code appeared 1.9% of the time in radiology billing in 2023 and helps evaluate abdominal pain and check for abnormalities in internal organs.
CPT 74183
74183 represents a CT scan of the abdomen and pelvis with contrast material. The contrast helps create more detailed images, making it easier to identify issues that might not show up on a non-contrast scan.
CPT 76700
76700 covers complete abdominal ultrasounds with real-time imaging. When billing this code, your documentation must include images of the upper abdominal aorta, liver, pancreas, spleen, kidneys, inferior vena cava, common bile ducts, and gallbladder. Missing any of these elements can result in claim denials.
CPT 73502
73502 bills for radiologic examination of the hip and pelvis, typically with two to three views. This code was reported 1.4% of the time in 2023 and helps diagnose hip fractures, arthritis, and other joint problems.
CPT 73030
73030 represents shoulder X-rays with at least two views. With shoulder injuries being common in both sports and workplace accidents, this code sees regular use at imaging centers.
CPT 74018
74108 covers abdominal X-rays with a single view of the organs and structures. This basic procedure was the 16th most used CPT code in 2023, often ordered to assess for bowel obstructions, perforations, or foreign objects.
How Do Professional and Technical Components Work?
 Here’s where radiology billing gets a bit more detailed. Most radiology services actually consist of two separate parts: the technical component and the professional component. Knowing how to bill these components correctly is critical for proper reimbursement.
Here’s where radiology billing gets a bit more detailed. Most radiology services actually consist of two separate parts: the technical component and the professional component. Knowing how to bill these components correctly is critical for proper reimbursement.
The technical component (TC) includes all the equipment, supplies, staff, and facility costs associated with performing the imaging procedure. When a hospital or imaging center owns the equipment and employs the technicians who perform the scan, they bill for the technical component by adding modifier TC to the CPT code.
The professional component (PC) covers the radiologist’s work in interpreting the images and writing the report. When a radiologist reads the films but doesn’t own the equipment or facility, they bill for the professional component by adding modifier 26 to the CPT code.
For example, let’s say a patient gets a chest X-ray at a hospital. The hospital provides the X-ray equipment, the radiology technician, and the room where the procedure happens. The hospital bills CPT code 71046-TC for the technical component. Meanwhile, a radiologist reviews the images and writes an interpretation report. That radiologist bills CPT code 71046-26 for the professional component.
The payment typically splits with approximately 60% going to the technical component and 40% going to the professional component. This split reflects the higher costs of maintaining equipment and facilities compared to the physician’s interpretation work.
When a single provider owns the equipment and also interprets the images, they bill the global service. This means submitting the CPT code without any modifier, which pays for both components together. For instance, if an orthopedic surgeon takes and interprets X-rays in their own office, they would bill the code globally without modifiers 26 or TC.
Which Modifiers Are Essential in Radiology Billing?
Beyond the TC and 26 modifiers, radiology billing uses several other modifiers that provide important details about the service performed.
- Modifier 50 (Bilateral Procedure): When the same procedure is performed on both sides of the body during the same session, append modifier 50. For example, bilateral knee X-rays would use modifier 50 to indicate both knees were imaged.
- Modifier RT (Right Side) and Modifier LT (Left Side): These anatomical modifiers specify which side of the body was examined when only one side received the service. Clear documentation prevents confusion and reduces denials.
- Modifier 76 (Repeat Procedure by Same Physician): When the same physician needs to repeat a procedure on the same day, modifier 76 tells the payer this wasn’t a billing error but a medically necessary repeat.
- Modifier 77 (Repeat Procedure by Another Physician): Similar to modifier 76, but used when a different physician performs the repeat procedure.
- Modifier 52 (Reduced Services): Sometimes only a portion of a procedure is performed. For instance, if a code calls for supervision and interpretation but only the interpretation is provided, modifier 52 indicates the service was reduced. Remember to also include modifier 26 in this case since you’re billing only the professional component.
- Modifier 53 (Discontinued Procedure): If a procedure must be stopped due to patient safety or other circumstances after it has begun, modifier 53 documents this situation. Don’t use this modifier if the procedure never started.
- Modifier 59 (Distinct Procedural Service): This modifier indicates that a procedure was separate and distinct from other services performed on the same day. Use it carefully and only when documentation clearly supports that the services were independent of each other.
When using multiple modifiers on a single code, radiology practices commonly combine them. For example, you might see modifiers 26, 59, and RT used together when appropriate. The key is ensuring your documentation supports every modifier you append to the claim.
What Documentation Do You Need for Radiology Claims?
 Proper documentation makes or breaks radiology claims. Insurance companies require specific elements before they’ll process your claim and issue payment.
Proper documentation makes or breaks radiology claims. Insurance companies require specific elements before they’ll process your claim and issue payment.
Every radiology claim needs a diagnosis code explaining why the procedure was medically necessary. These ICD-10 codes describe the patient’s symptoms, condition, or disease that prompted the imaging study. Non-specific diagnosis codes often trigger denials, so be as precise as possible based on the clinical information available.
When billing for “complete” procedures, your documentation must prove you actually performed the complete exam. Remember the earlier example of CPT code 76700 for a complete abdominal ultrasound? If your records don’t include images and assessment notes for every required organ and structure, your claim for the complete procedure will be denied.
For procedures using contrast materials, clearly document whether single or double contrast was used. Different codes apply depending on whether contrast was administered, so accurate documentation ensures correct code selection.
The physician order is another essential piece. Medicare and most commercial payers require documentation showing that an appropriate provider ordered the imaging study. The ordering physician’s name, NPI number, and the clinical reason for the order should all be clearly documented.
Your radiology report should include all standard elements: patient demographics, procedure performed, technique used, findings, and the radiologist’s interpretation. The report serves as the official record of what was done and what was discovered, so completeness and accuracy matter tremendously.
What Common Billing Errors Should You Avoid?
Even experienced billing staff make mistakes with radiology codes. Being aware of common pitfalls helps you avoid costly errors.
- Upcoding happens when you bill at a higher level than the service actually provided. For example, billing for a CT scan with contrast when only a non-contrast scan was performed inflates reimbursement inappropriately and can lead to audits and penalties.
- Undercoding is the opposite problem. Billing for a lower-level service than what was actually performed means you lose revenue that you rightfully earned. If a patient receives a CT scan with contrast but you bill for a non-contrast scan, you’re leaving money on the table while undervaluing the service provided.
- Missing modifiers cause claim denials and payment delays. When you fail to append modifier 26 or TC to indicate whether you’re billing the professional or technical component, payers can’t determine proper reimbursement. They’ll either deny the claim or request clarification, slowing down your payment cycle.
- Duplicate billing occurs when multiple providers bill for the same service without proper modifiers. If both the facility and the radiologist submit the global code instead of using TC and 26 modifiers, payers see duplicate claims and deny one or both.
- Incomplete documentation leads to denials even when the correct code is used. If you bill for a complete procedure but your records show only a partial exam, expect the claim to come back unpaid.
Wrong place of service causes problems particularly with modifier 26 claims. The place of service code on professional component claims should reflect where the procedure was performed, not where the radiologist read the images. Only certain place of service codes are appropriate for TC and PC billing.
How Do New Technology and AI Impact Radiology Billing?
 The radiology field continues advancing rapidly, and these changes affect billing practices. Electronic health record systems now often include built-in coding assistance to help prevent common errors. These systems can suggest appropriate codes based on procedure descriptions and clinical documentation.
The radiology field continues advancing rapidly, and these changes affect billing practices. Electronic health record systems now often include built-in coding assistance to help prevent common errors. These systems can suggest appropriate codes based on procedure descriptions and clinical documentation.
Computer-aided coding tools analyze imaging reports and recommend appropriate codes, making the billing process more efficient. However, human oversight remains essential. Technology can suggest codes, but experienced coders must verify that the suggestions match the actual service performed and the documentation provided.
Artificial intelligence is beginning to play a role in radiology billing. Some systems can now analyze imaging reports and automatically suggest appropriate codes based on the procedures described and findings documented. While this technology shows real promise for reducing coding errors and speeding up the billing process, it’s not yet sophisticated enough to replace human judgment entirely.
The American Medical Association updates CPT codes annually, adding new codes for emerging technologies and retiring outdated ones. For 2025, the American College of Radiology announced several new and updated Category I codes. Staying current with these changes is critical because using outdated codes leads to claim denials.
What Role Does Prior Authorization Play?
Many insurance companies now require prior authorization for certain radiology procedures, particularly advanced imaging like MRIs, CT scans, and PET scans. This means you must get approval from the payer before performing the procedure, or risk not getting paid.
Prior authorization requirements vary widely by payer and even by specific insurance plan. Some payers require authorization for all advanced imaging, while others only require it for certain anatomical areas or when specific clinical criteria aren’t met.
Failing to obtain required prior authorization is one of the fastest ways to get a claim denied. The procedure might have been medically necessary and properly performed, but without that prior approval, many payers will refuse payment. Your practice then faces the difficult position of either writing off the charge or attempting to collect from the patient, which can damage patient relationships.
Building prior authorization checks into your scheduling process helps avoid these problems. Before scheduling high-cost imaging procedures, verify whether authorization is needed and obtain it if required. Track authorization numbers and include them on claims to smooth the payment process.
How Can You Improve Your Radiology Billing Operations?
![]() Given the intricacies of radiology coding and billing, many practices struggle to keep up with claim submissions, denials, and follow-up. Errors in coding or documentation lead to denied claims, delayed payments, and lost revenue. Even small mistakes add up when you’re dealing with hundreds or thousands of imaging procedures each month.
Given the intricacies of radiology coding and billing, many practices struggle to keep up with claim submissions, denials, and follow-up. Errors in coding or documentation lead to denied claims, delayed payments, and lost revenue. Even small mistakes add up when you’re dealing with hundreds or thousands of imaging procedures each month.
Staying current with annual CPT code updates, payer-specific requirements, and changing regulations requires significant time and expertise. Your clinical staff is focused on providing excellent patient care and producing high-quality diagnostic images. Adding billing responsibilities to their workload often leads to mistakes and burnout.
This is where specialized support makes a real difference. At Medwave, we handle medical billing, credentialing, and payer contracting for healthcare providers, including radiology practices. Our team stays current with the latest coding updates, modifier requirements, and payer policies so you don’t have to. We handle everything from initial claim submission through denial management and appeals, working to maximize your reimbursement while reducing your administrative burden.
Whether you need help with your entire revenue cycle or just want support with specific aspects like coding or credentialing, partnering with experts who specialize in radiology billing can improve your cash flow, reduce claim denials, and free up your staff to focus on patient care.